

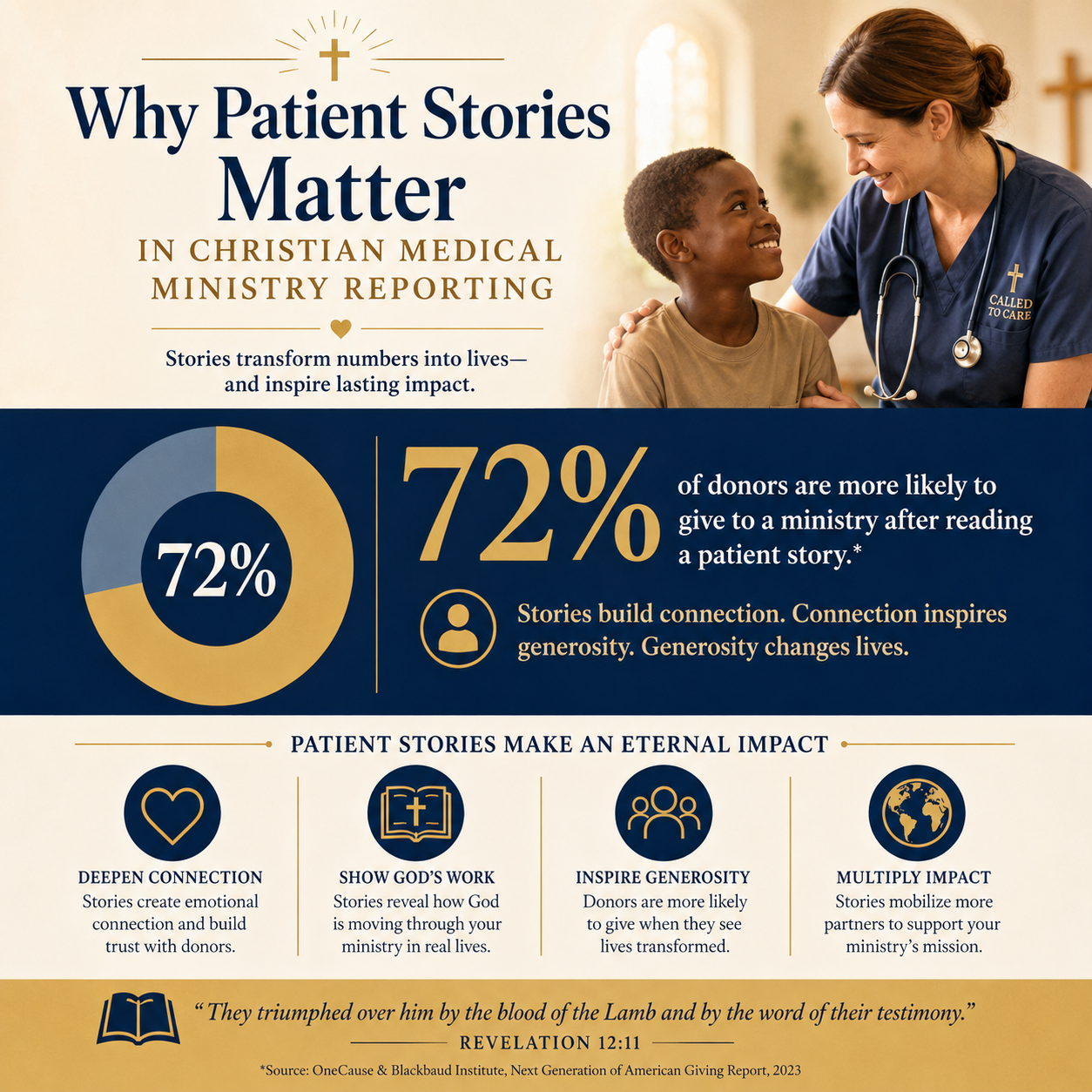
Patient stories matter in Christian medical ministry reporting because they answer the question serious donors are already asking: what kind of healing is taking place, and is it consistent with the character of Christ? A clinic count can tell us volume, and a budget can tell us capacity. Neither can, by itself, tell us whether a ministry is treating people as image-bearers or merely processing need.
Scripture does not separate bodily care from moral seriousness. Jesus’ ministry included healing and also restored people to community, dignity, and worship. Christian donors, therefore, are right to expect reporting that reflects both compassion and truth. Patient stories, carefully gathered and responsibly told, are one of the few tools that can illuminate outcomes, surface ethical risks, and keep ministries accountable to their stated faith commitments.
Patient stories connect impact to the image of God
Reporting that honors persons, not projects
Christian medical work is never only a technical intervention. It is care offered to someone who bears God’s image and whose suffering has moral weight. Numbers can quantify services rendered; they cannot, on their own, reveal whether care was offered with respect, consent, and appropriate follow-through. A patient story can show whether a mother understood her treatment plan, whether a child’s guardian was counseled well, whether the staff treated an uninsured laborer with the same attention given to a paying patient.
Donors often feel the tension here. We want verifiable evidence, and we also want to know whether a ministry’s compassion is more than a slogan. Patient stories, when they are not curated into propaganda, can reveal the spiritual posture behind the clinical work: humility, patience, truth-telling, and refusal to exploit vulnerability for fundraising.
Why the Gospels still set the standard
The Gospels routinely name individuals rather than only crowds. Jesus touches lepers, speaks to a Samaritan woman, and addresses blind men who cry out for mercy. This is not sentimentality; it is theological realism. God relates to persons. Reporting that never descends from aggregate totals to human particularity can quietly train donors to think of care as an abstract commodity rather than an act of mercy rendered to a neighbor.
In our work at Most Trusted, we see that ministries with a durable faith foundation tend to treat reporting as an extension of discipleship: speech that is truthful, restrained, and mindful of power. Patient stories are one of the clearest places where that maturity shows.

Stories make outcomes intelligible, not merely impressive
From activities to meaningful change
Healthcare reporting is often crowded with activity metrics: consultations, surgeries, days of inpatient care, prescriptions dispensed. These have value, but donors are increasingly aware that volume can coexist with weak outcomes. A large outreach event can mask inadequate follow-up. A high surgery count can conceal complications. A story can clarify what an “outcome” actually meant in that context: functional recovery, adherence to treatment, restored ability to work, reduced pain, or a safe referral when the ministry’s own capacity was limited.
This is where responsible narrative belongs alongside clinical realism. A story that names constraints—medicine stock-outs, staffing limits, distance to referral hospitals, or cultural barriers to follow-up—often increases credibility. Mature donors are not looking for perfection. They are looking for ministries that tell the truth and improve.
Why donors should be wary of the single triumphant testimony
Christians genuinely disagree about how much testimony belongs in public reporting. Some ministries lean heavily on dramatic healings and conversions; others avoid spiritual claims altogether to protect patients or local partners. Both instincts can be principled. The problem is not testimony. The problem is selection bias: if only the most dramatic stories are told, donors can develop a distorted sense of typical results and underestimate the ordinary faithfulness of long-term care.
Well-constructed reporting uses stories to explain the ministry’s theory of care, not to bypass evaluation. In practice, that means pairing narrative with sober context: what proportion of patients receive follow-up, how complications are handled, and when the ministry refers patients elsewhere. For donors tracking ministries in Christian Medical Ministries, stories become most useful when they clarify what the numbers cannot say and do not attempt to replace the numbers.
Stories can strengthen transparency, but they can also create ethical risk
Consent and privacy are not optional virtues
Medical storytelling carries a moral hazard that Christian donors should name directly: people in crisis are easily exploited. A patient may feel pressure to consent to a photo, an interview, or a public testimony because the ministry has resources they need. Even when consent forms are used, power dynamics can make “yes” ambiguous.
Healthcare ethics offers important guardrails here, and Christian reporting should exceed them rather than skirt them. In the United States, privacy expectations are reinforced by HIPAA, a federal health information privacy framework administered by the U.S. Department of Health and Human Services HHS HIPAA. International settings differ legally, but the moral principle is stable: ministries should not treat a patient’s pain as a communications asset.
Depicting suffering without manufacturing dignity
Some reporting practices appear compassionate but subtly degrade the people they claim to serve. The field has had to reckon with “poverty pornography,” a critique that applies equally to medical imagery when it reduces patients to wounds, tears, and desperation. Christian donors should not accept storytelling that trades in humiliation to secure sympathy.
Responsible ministries tend to adopt clear internal standards: using de-identified descriptions when risk is high, avoiding before-and-after framing that objectifies bodies, and ensuring local leadership has genuine authority over how patient narratives are shared. These practices align with the transparency donors seek without surrendering dignity for attention.
- Clear, non-coercive consent processes in the patient’s primary language
- Privacy protections that limit identifying details unless truly necessary
- Local clinical leaders empowered to veto story requests
- A preference for “patient voice” over staff interpretation when appropriate
- Policies that prevent fundraising deadlines from driving clinical storytelling
Stories help donors evaluate stewardship under The Most Trusted Standard
What narratives reveal about governance and leadership
Many donors have learned that financial statements and program totals are necessary but insufficient. Governance is tested in what an organization rewards and what it refuses to do. Patient stories can reveal whether a ministry has mature leadership habits: careful review processes, clear accountability for communications, and a willingness to report limitations without fear.
At Most Trusted, our verification work is organized around The Most Trusted Standard, a 15-criteria framework across Faith Foundation, Financial Integrity, Governance and Leadership, and Transparency and Effectiveness. Patient stories are not a criterion by themselves, but they often function as diagnostic evidence. A ministry that tells patient stories with integrity usually has other disciplines in place: documented policies, responsible oversight, and a culture that treats truthfulness as part of Christian witness.
When stories substitute for evidence
The harder question is how donors should respond when a ministry offers abundant stories but little verifiable reporting. Story-only communication can become a way to avoid accountability, especially when an organization is unwilling to share basic information about outcomes, safeguarding, or financial integrity.
Christian donors should also be alert to the opposite error: demanding a kind of measurement that a small or rural clinic cannot reasonably produce without diverting clinical capacity. The aim is proportional evidence—reporting that is rigorous enough to be trustworthy and feasible enough to be sustainable. This is one reason we encourage donors to assess ministries within a coherent framework rather than using one metric as a proxy for faithfulness. Many of these donor questions sit within How Christian Medical Ministries Measure Impact, where narrative and measurement should be treated as complementary rather than competitive.
Better storytelling is a form of neighbor love
How ministries can tell the truth without exaggeration
Christian storytelling should be governed by the command not to bear false witness and by the obligation to love our neighbor. That combination produces a particular kind of reporting: specific but restrained, compassionate but accurate, careful about claims, and unwilling to overstate causality. A patient’s improvement may be partly due to the ministry’s care and partly due to factors outside the ministry’s control. A credible story can name that without diminishing gratitude.
Donors can encourage this by rewarding ministries that report in sober tones. When donors only celebrate the most dramatic narratives, ministries are incentivized to select, polish, and amplify rather than to tell the truth. Better incentives produce better reporting.
How donors can read stories with spiritual and practical discernment
Patient stories should move Christian hearts, but they should also train Christian judgment. We recommend reading stories with a few disciplined questions in mind: Does the patient retain agency in the telling, or are they spoken about? Does the story clarify follow-up, referrals, and limits of care? Does it avoid implying that medical care was contingent on spiritual response? Does it fit plausibly with the ministry’s stated capacity and budget?
Discernment is not cynicism. It is stewardship. The same love that compels generosity also requires careful attention to truth, because distorted reporting ultimately harms patients and misleads the church.
FAQs for Why patient stories matter in Christian medical ministry reporting
Should Christian medical ministries report patient stories at all, given privacy concerns?
Yes, but only with safeguards strong enough to protect the patient’s dignity and confidentiality. Non-coercive consent, careful de-identification where appropriate, and clinical leadership authority over storytelling are basic expectations. Donors should treat privacy as part of Christian ethics, not as a public-relations detail.
What should donors do when a ministry shares powerful stories but little measurable reporting?
We recommend asking for additional evidence that can be verified: follow-up practices, referral relationships, safeguarding policies, financial statements, and leadership oversight of communications. Stories can illuminate meaning, but they cannot replace accountability. Ministries worthy of long-term partnership typically welcome careful questions.
Patient stories as truthful witness
Christian medical ministry reporting should make suffering visible without exploiting it, and it should make outcomes intelligible without exaggeration. Patient stories matter because they can bear truthful witness to the kind of care being offered—care that recognizes the image of God, protects the vulnerable, and refuses to trade dignity for donations. When narrative is governed by truth and love, it becomes one of the most credible forms of transparency available to the church.



