
How Christian medical ministries balance program and operating costs is not a cosmetic accounting question. It is a spiritual and fiduciary question about whether a ministry is building durable capacity to love the sick well, or whether it is starving the very systems that make faithful care possible. Donors rightly want the maximum share of a gift to reach patients, yet Scripture’s vision of stewardship is not a contest to minimize administration; it is a call to be found faithful with what belongs to God.
Christian donors often inherit a simple rule of thumb: “low overhead equals high impact.” The field has had to reckon with how misleading that can be. In 2013, the leaders of Charity Navigator, GuideStar, and the BBB Wise Giving Alliance publicly warned against using overhead ratios as a primary indicator of charity performance, noting that pressure to minimize overhead can undercut effectiveness and transparency. BBB Wise Giving Alliance
Program versus operating is a moral distinction but not a holy one
Mercy to bodies requires systems, not only compassion
Christian medical work lives close to Matthew 25’s summons to visit the sick and to treat the vulnerable as we would treat Christ. The New Testament never presents mercy as disorganized improvisation. The early church appointed leaders to administer food distribution because neglect and inequity were appearing in daily operations (Acts 6). The principle remains: faithful care requires structures that prevent predictable failures.
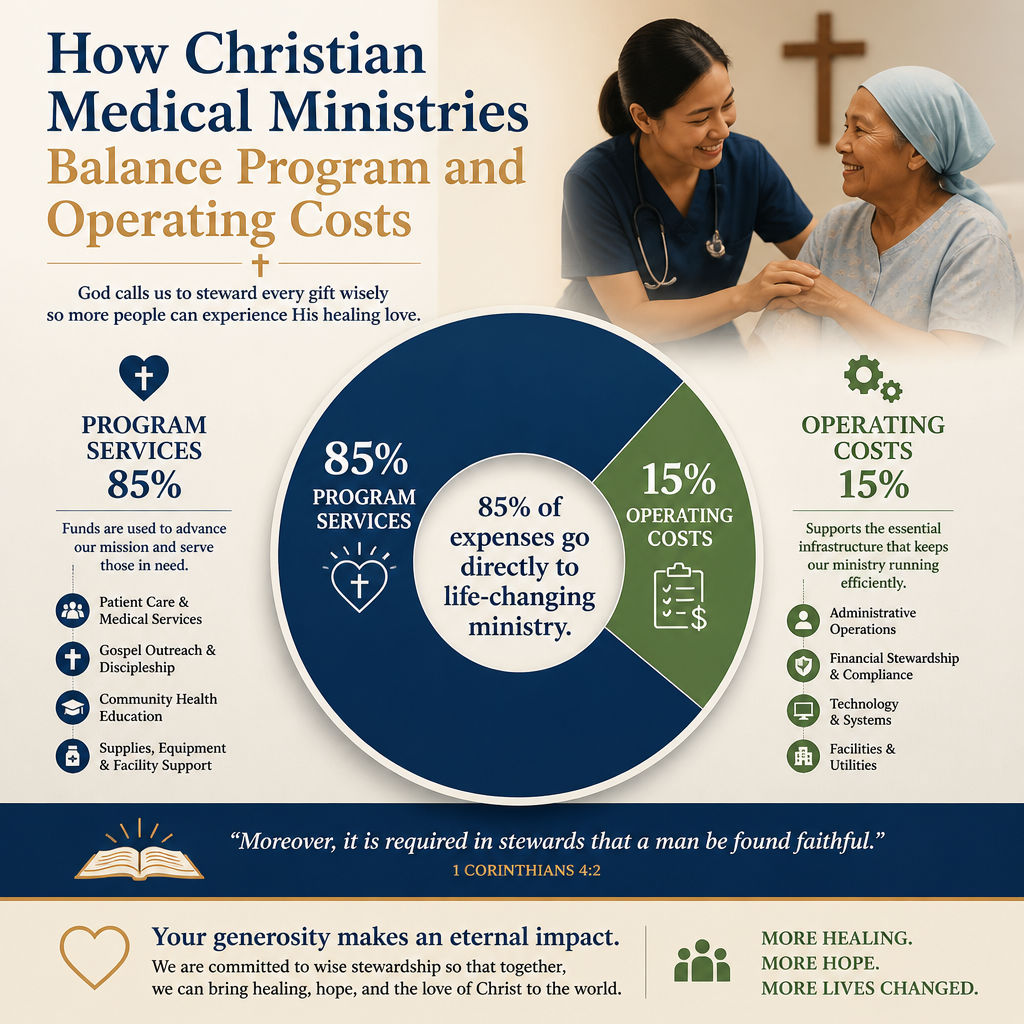
Program costs and operating costs are both means toward a single end: ministry that is truthful, competent, and durable. In clinical work, the “operating” side often includes credentialing, safeguarding, medication control, cold-chain management, infection prevention protocols, audit trails for restricted gifts, cybersecurity for patient data, and training in ethical care. When those functions are underfunded, the ministry may appear lean while becoming brittle.
Accounting categories do not always map cleanly to mission
The same activity can be categorized differently depending on context and accounting policy. A nurse supervisor who spends half her week training clinicians might be coded as “program” by one ministry and “management” by another. A development director coordinating major gifts for a maternal health clinic may be labeled “fundraising,” yet the ability to fund the clinic is inseparable from whether the clinic remains open.
Christians genuinely disagree about where to draw lines. The wiser question is not whether a ministry can tell a donor that overhead is “only” a certain percentage. The wiser question is whether the ministry’s allocation reflects integrity, competence, and a refusal to manipulate categories to satisfy donor pressure.

Why medical ministry overhead can be higher without being wasteful
Clinical quality and patient safety are labor intensive
Medical work carries risks that other forms of aid do not. A poorly stocked pharmacy, an inadequately trained clinician, or a failure in sterilization is not merely inefficiency; it can harm the people the ministry is called to serve. That reality changes what “responsible operations” must include, especially as ministries move from episodic outreach toward longitudinal care.
Regulatory compliance, even when a ministry operates outside the United States, often still involves credible standards: professional licensing, controlled substance rules, facility inspections, and referral relationships. Those responsibilities are frequently housed in “operations” or “management” lines, but they are part of loving one’s neighbor with competence.
Supply chains and infrastructure are mission-critical, not optional
Many Christian medical ministries serve in environments with fragile logistics. Fuel shortages, port delays, counterfeit medications, and disrupted communications can turn a well-funded program into a non-functioning one. Operations teams build supplier relationships, redundancy, and verification processes that protect patients.
Donors can also underestimate the costs of measurement that are ethically required. Collecting accurate clinical outcomes, reporting adverse events, and documenting patient consent are not distractions from ministry; they are expressions of truthfulness, and truthfulness is not negotiable in Christian witness.
The danger is not overhead itself but the starvation cycle
Underfunded operations often create hidden costs and moral compromises
Pressure to keep overhead artificially low can tempt ministries into practices that are not worthy of Christian stewardship: delaying technology upgrades until a breach forces change, paying below-market wages that produce constant turnover, or avoiding evaluation so that difficult outcomes remain unseen. These are not merely tactical errors. They can become forms of untruth, because the ministry presents itself as strong while quietly eroding the foundations needed for safe care.
This dynamic is widely recognized in philanthropy as the “nonprofit starvation cycle,” in which restricted funding and donor expectations drive chronic underinvestment in infrastructure and capacity. The analysis is often associated with Ann Goggins Gregory and Don Howard’s work in Stanford Social Innovation Review. Stanford Social Innovation Review
Overhead minimization can conflict with the duty to be transparent
In Christian giving, the desire to “send every dollar to the field” can be spiritually sincere. It can also become a form of sentimentality if it refuses to face what real medical care costs. When donors demand a number rather than a truthful picture, ministries may respond by placing ordinary operating expenses into program lines, or by keeping systems informal to avoid costs that would be visible. The result is often less accountability, not more.
Across our verification work at Most Trusted, the ministries that meet The Most Trusted Standard tend to treat financial clarity as part of discipleship: they explain their cost structure without defensiveness, and they resist simplistic marketing that implies overhead is inherently suspect.
What healthy cost balance looks like in practice
Signs that operations are serving mission rather than consuming it
Mature Christian medical ministries usually show a consistent pattern: they invest enough in operations to protect patients and staff, they control growth rather than chasing scale, and they can explain how each major cost category connects to safe and effective care. They also present fundraising as a legitimate ministry function rather than as a necessary evil.
Donors should not be asked to accept vague assurances. They should be able to see evidence: audited financial statements when appropriate, clear allocation methodologies, and reporting that does not confuse storytelling with outcomes. In the language of The Most Trusted Standard, financial integrity and transparency are not compliance exercises; they are part of truthful witness.
Questions donors can ask without forcing ministries into performative frugality
The most helpful donor questions are specific, contextual, and difficult to game. They press toward governance, controls, and patient safety rather than toward a single ratio.
- How does the ministry define and allocate program, management, and fundraising costs, and is the methodology consistent year to year?
- What internal controls exist for cash handling, restricted gifts, and procurement, especially for medications and equipment?
- How does leadership evaluate clinical quality, patient safety, and outcomes, and what happens when results are disappointing?
- What proportion of staff are retained year to year, and what is the plan for training and succession in key roles?
- What does the ministry do to prevent harm, including safeguarding, informed consent, and appropriate referral pathways?
For donors comparing organizations in this space, our team encourages reading within the broader context of Christian Medical Ministries, where the central question is not only what a ministry spends, but what its spending reveals about its faithfulness under pressure.
How verification helps donors discern faithful stewardship
Ratios can be a prompt, but never the verdict
Expense ratios can still serve a purpose. A sudden spike in fundraising costs, persistent operating deficits, or highly inconsistent allocations can be warning signs. But a verdict requires more than arithmetic. It requires governance context, clarity about revenue mix, and an understanding of the ministry’s stage of growth. A newer clinic expanding services may carry heavier administrative costs for a season; the question is whether leadership is honest about why, and whether the investment is producing healthier operations over time.
Wise donors also distinguish between “inefficiency” and “capacity.” A well-run clinical training program may look like overhead to a casual reader of a Form 990, while it actually prevents medical errors and raises quality across years of service.
What The Most Trusted Standard aims to clarify
Most Trusted exists because discerning donors need more than marketing claims. We evaluate Christian nonprofits against The Most Trusted Standard, a 15-criteria framework that examines faith foundation, financial integrity, governance and leadership, and transparency and effectiveness. In medical ministry, these areas converge quickly: a theology of human dignity demands ethical clinical practice; ethical clinical practice requires governance; governance requires competent operations; and competent operations require honest funding.
Within How Christian Medical Ministries Use Donations, we consistently see that the strongest ministries do not apologize for necessary operating expenses. They explain them, govern them, and subject them to oversight so that donors can give with confidence and the sick can receive care without unnecessary risk.
FAQs for How Christian medical ministries balance program and operating costs
What overhead percentage should a Christian medical ministry have?
There is no single faithful percentage that fits every medical ministry. The better standard is whether operating costs are governed, explained, and proportionate to the complexity and risk of the services provided. The 2013 public statement from Charity Navigator, GuideStar, and BBB Wise Giving Alliance cautioned donors against using overhead ratios as the primary measure of performance because it can incentivize underinvestment in effectiveness and accountability. GuideStar
Is fundraising an acceptable expense for a ministry that serves the sick?
Fundraising is acceptable when it is truthful, proportionate, and governed. A medical ministry that depends on donations must communicate with supporters, steward donor intent, and build durable revenue. The ethical questions are whether fundraising claims are accurate, whether costs are controlled, and whether appeals manipulate emotion rather than tell the truth. Faithful stewardship does not treat fundraising as inherently unspiritual; it subjects it to integrity.
Giving that strengthens care rather than merely counting dollars
Christian medical ministries balance program and operating costs well when they refuse both waste and performative austerity. The aim is not to defend overhead, but to fund the full reality of safe, truthful, durable medical care—care that honors the image of God in patients, protects the vulnerable from harm, and allows a ministry to endure beyond a single campaign. Donors serve that end best when they insist on clarity, governance, and verifiable integrity rather than a single reassuring ratio.



