
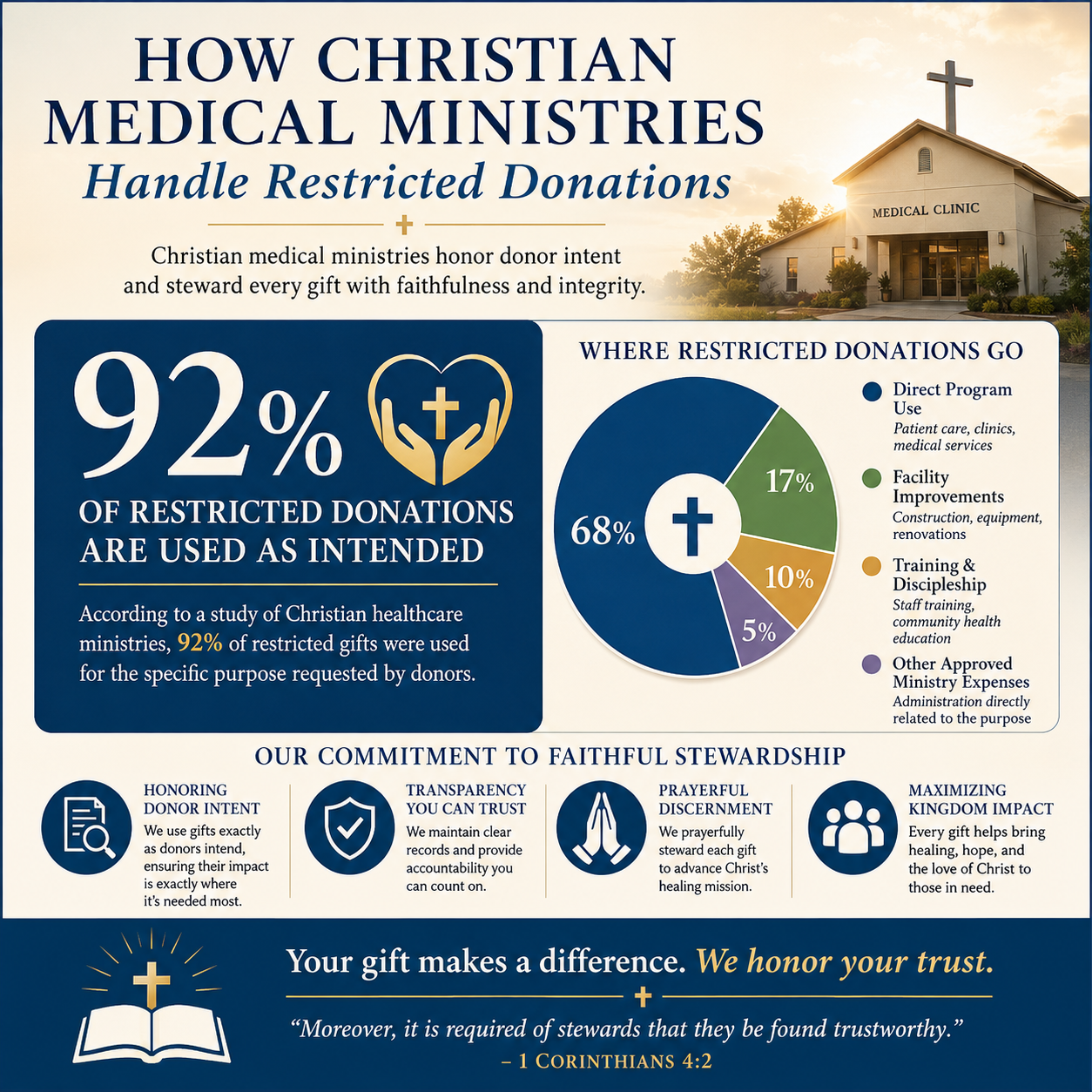
How Christian medical ministries handle restricted donations is one of the clearest tests of whether a ministry treats donors as partners in stewardship or merely as funding sources. When a gift is restricted, the question is not simply administrative; it is moral and theological, because “it is required of stewards that they be found faithful” (1 Corinthians 4:2). Faithfulness here means honoring donor intent, telling the truth about what a gift can and cannot do, and refusing the subtle temptation to use sacred language to cover ordinary budget pressure.
Most Christian donors understand the urgency of medical work. A hospital shipment delayed by customs, a clinic refrigerator that fails, or a child whose surgery cannot wait does not feel like a line item. Yet urgency can also become the rationale for bending restrictions “just this once.” Mature ministries resist that logic. They build systems that allow compassion to remain compassionate without becoming careless.
Restricted gifts are promises, not preferences
Donor intent is a form of truth telling
A restricted donation is a donor’s instruction that funds be used for a specified purpose: cataract surgeries, rural prenatal care, a mobile clinic, a tuberculosis program, a medical training institute, or a particular country. The restriction may be formal in a grant agreement or simple in a donation form selection, but the ethical weight is the same. The donor is not merely expressing interest; the donor is establishing a condition of the gift.
Scripture treats vows and pledged commitments with sobriety. The point is not legalism; it is integrity. When a ministry accepts a restricted gift and later redirects it because “needs changed,” the ministry is effectively rewriting the promise after receiving the money. That is not nimble ministry. It is a breach of trust, even when the alternative use is genuinely good.
Restricted giving is common and increasingly complex
In healthcare missions, restrictions multiply because the work is naturally programmatic: medicines, procedures, equipment, and care delivery are tangible and easily designated. Many donors also restrict gifts because they have learned—sometimes through hard experience—that general funds can disappear into overhead without clear connection to outcomes. That concern is not always fair, but it is common.
The field has also had to reckon with how simplistic “overhead” narratives mislead donors. The “Overhead Myth” statement—signed by leaders from GuideStar (now Candid), BBB Wise Giving Alliance, and Charity Navigator—argued that focusing on overhead ratios can starve organizations of the infrastructure needed for effectiveness and accountability https://www.candid.org/. Christian medical ministries that handle restricted gifts well address this directly: they do not shame donors for caring about efficiency, but they also teach donors why strong finance systems, compliance, and clinical quality controls are not optional.

How responsible medical ministries accept restrictions
They clarify what the restriction means before taking the money
The most reliable ministries treat restricted funds as a front-end conversation, not a back-end problem. That means they define the program, geography, population, and time horizon with enough specificity that both parties can recognize compliance. If a donor writes “for medical care,” that may function as general program support. If the donor writes “for pediatric oncology in northern Uganda,” the ministry must be able to track both purpose and location and to report accordingly.
Across our verification work at Most Trusted, we observe that the ministries that meet The Most Trusted Standard tend to have written gift acceptance policies that address restrictions explicitly: what they can accept, what they will not accept, and what happens if circumstances change. This is not bureaucracy for its own sake. It is the difference between predictable stewardship and improvisation under pressure.
They assess feasibility, compliance, and clinical integrity
Restricted medical gifts can create risks that donors do not always see. A donation restricted to “surgical missions” may imply short-term trips that lack continuity of care. A gift restricted to “free medicines” can undermine local markets or encourage dependency if not coordinated with local providers. The When Helping Hurts framework, articulated by Steve Corbett and Brian Fikkert, has helped many Christian organizations name these dynamics without abandoning compassion.
Responsible ministries therefore ask hard questions before accepting a restriction: Does this fit our model of care? Can we maintain medical standards? Can we procure ethically? Can we follow local law? If the answer is no, the honest response is to decline the restriction or request a modification, not to accept the money and “figure it out later.”
How restricted funds are tracked, spent, and reported
Separate accounting is necessary, but not sufficient
At a minimum, restricted funds require fund accounting that prevents commingling and documents expenditures against the designated purpose. Many ministries use accounting software that allows restrictions by fund, project, and location. The point is auditability: a ministry should be able to show, with transactions and supporting documents, that a restricted gift was spent as promised.
But accounting alone does not ensure faithful use. In medical work, the most consequential failures are often operational: supplies purchased but not delivered, equipment donated but never maintained, or services reported without sufficient documentation. Strong ministries connect finance systems to program controls—inventory logs, clinical records protocols, procurement policies, and supervisory review—so that restricted spending aligns with real care delivered.
Reporting should serve truth, not marketing
Restricted gifts invite program reporting, and program reporting can drift into promotional storytelling. Mature reporting is concrete: what was done, for whom, where, and with what limitations. It should include setbacks as well as progress, especially in medical contexts where complications, supply chain disruptions, and staffing shortages are part of reality.
Christians genuinely disagree about the best way to measure outcomes in mission healthcare. Some emphasize spiritual fruit and local church partnership. Others prioritize clinical metrics such as patient follow-up, infection rates, referral pathways, and continuity of care. Responsible ministries do not collapse the disagreement with slogans. They articulate what they measure and why, and they avoid implying that numbers alone capture faithfulness.
- Clear restriction language that a donor can understand and a finance team can code
- Fund-level tracking that prevents restricted dollars from covering unrelated expenses
- Documented approvals for expenditures tied to the restriction
- Program evidence that connects spending to actual services delivered
- Donor reporting that is specific, timely, and candid about constraints
Donors who want to go deeper into the wider stewardship patterns in the sector often begin with Christian Medical Ministries, because restricted giving makes sense only in the context of how a ministry actually operates.
When restrictions collide with real-world medical needs
Changed circumstances require consent, not creativity
Healthcare is volatile. A ministry may receive a restricted gift for a clinic in one region and then face political instability that closes the clinic. A donor may restrict a gift to a medication that becomes unavailable or medically outdated. In these cases, ethical practice is not “closest purpose” spending without notice. Ethical practice is to seek donor consent to redirect funds, or to hold the funds until the restriction can be honored, or to return the gift if neither option is workable.
This is where governance matters. A board that treats restrictions as a mere finance detail will tend to accept quiet reallocations when budgets tighten. A board that understands fiduciary duty and Christian witness will require documentation, donor communication, and clear internal controls. Those are not secular add-ons; they are part of what it means for Christian organizations to “provide things honest in the sight of all men” (Romans 12:17, KJV).
Emergency appeals can unintentionally create restricted-fund backlogs
Medical ministries often fundraise through urgent, designated appeals: “sponsor a surgery,” “send a doctor,” “deliver a container of medicine.” These appeals can be appropriate, but they can also create a mismatch between what is funded and what can be delivered in a given quarter. A backlog of restricted cash may look healthy in the bank, while the ministry struggles to cover core staffing, compliance, and follow-up care.
The harder question is whether a ministry is willing to tell donors that general support sometimes saves more lives than designated gifts. Done poorly, this becomes a manipulative pitch for “unrestricted because we say so.” Done well, it is a sober explanation of what makes medical work safe and sustainable: clinical supervision, training, equipment maintenance, patient records, and local partnerships. Donors are often more willing to fund these essentials when a ministry has earned credibility through transparency.
What discerning donors should ask before restricting a medical gift
Restrictions can be an act of care, or a substitute for trust
Some donors restrict because they have a clear calling: maternal health, disability care, or trauma surgery. Others restrict because they are unsure whether the ministry will use general funds wisely. The first impulse can be faithful focus. The second impulse may signal that the donor needs more information—or a different ministry.
At Most Trusted, our work is to reduce the need for guesswork by evaluating ministries against The Most Trusted Standard across faith commitments, financial integrity, governance, and transparency. Donors still must exercise discernment, but they should not have to rely on glossy reports or emotional appeals to know whether restrictions will be honored.
Practical questions that reveal stewardship quality
Before making a restricted gift, donors can ask questions that are straightforward but revealing:
1) What happens if this project cannot be completed as described? The answer should include donor consent processes, not vague assurances.
2) How do you track restricted gifts in your accounting system? The answer should be specific enough that it could be audited.
3) Do you have a written gift acceptance policy? If not, restrictions will likely be handled ad hoc.
4) What clinical and operational safeguards are in place? Medical work requires quality controls beyond basic charitable compliance.
5) What portion of the work requires general support to sustain the restricted program? Honest ministries can explain the relationship between designated activities and the infrastructure that makes them safe.
For donors comparing approaches across organizations, How Christian Medical Ministries Use Donations is often where the real differences become visible, because spending patterns disclose governance and leadership quality over time.
FAQs for How Christian medical ministries handle restricted donations
Can a ministry use restricted donations for overhead or administrative costs?
Only if the restriction explicitly allows it or if the donor agrees in writing to a modification. Many donors use “overhead” imprecisely; certain administrative costs are directly necessary for medical care—billing systems, compliance, procurement controls, and clinical supervision. The ethical question is not whether such costs exist, but whether the ministry represented the gift accurately and can document that spending aligns with the donor’s stated purpose.
What should happen if a donor-restricted project becomes impossible?
The ministry should contact the donor with clear options: approve a revised use that remains close to the original intent, hold the funds until the project becomes feasible again, or return the gift. Quiet internal reassignment may feel efficient, but it undermines trust and can create legal exposure. A ministry that treats donor consent as indispensable is demonstrating both governance maturity and Christian integrity.
A credible ministry treats restrictions as discipleship-level stewardship
Restricted donations can be a gift to Christian medical ministries because they help donors participate in concrete works of mercy: caring for the sick, strengthening fragile health systems, and honoring the dignity of those who suffer. They can also become a source of distortion when ministries accept restrictions they cannot fulfill, report selectively, or reassign funds without consent.
The ministries worthy of long-term partnership handle restricted gifts with clarity, controls, and candor. They do not rely on sentiment to carry them through accountability. They treat each restriction as a promise made before God and neighbor, and they build governance and financial practices strong enough to keep that promise under pressure.



