
How Christian medical ministries use donations is a stewardship question before it is a budgeting question. Mature Christian donors are not merely asking whether a ministry is “efficient,” but whether its spending patterns align with a biblical account of mercy, truthfulness, and accountability before God.
Medical work sits at a moral intersection that makes spending scrutiny both necessary and complicated. The needs are visible and urgent, the logistics are expensive, and the public narratives can drift toward either suspicion (“overhead is waste”) or sentimentality (“any cost is justified”). Scripture pushes against both temptations. Jesus’ parable of the talents assumes measured responsibility with entrusted resources (Matthew 25:14–30). James insists that faith expresses itself in concrete care for those in distress (James 2:14–17). For donors, the question is how to give in a way that strengthens faithful care rather than funding poor incentives.
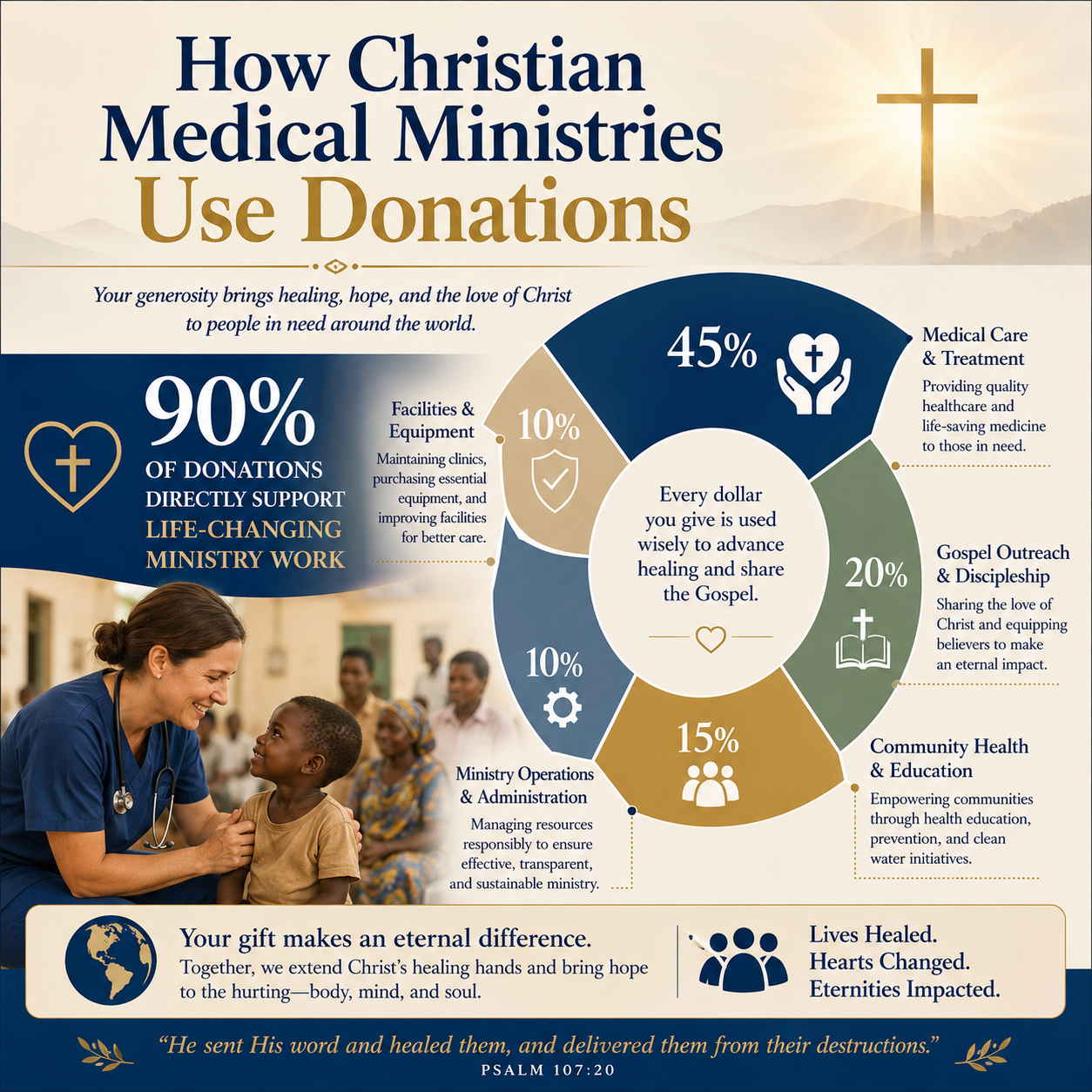
Donations fund more than medicine, because medicine is never only medicine
Christian medical ministries typically spend donor gifts across a set of interlocking functions. Direct clinical care is central, but it is rarely the only meaningful cost. The difference between “program” and “overhead” is not always the difference between mission and waste; it is often the difference between immediate service and the infrastructure that keeps patients safe, clinicians accountable, and outcomes verifiable.
Direct care can mean supplies, staffing, and service delivery
In some ministries, “direct medical care” means patient encounters in a clinic or hospital: clinician time, medication, diagnostics, and facility operations. In others, it means mobile medical teams, community health workers, or surgical trips carried out with local partners. In still others, it means financing care indirectly—covering treatment costs for patients who cannot pay, subsidizing a hospital ward, or underwriting a vaccination campaign.
The cost structure differs dramatically by setting. A U.S.-based free clinic, an East African rural hospital, and a disaster-response medical team face different compliance regimes, staffing markets, and supply-chain realities. Serious donors should expect those differences to show up in financial statements rather than demanding a single “right” ratio.
Capacity is not mission drift when it serves patient safety and dignity
Administrative systems are often the invisible difference between help and harm. Credentialing and supervision protect patients from unqualified practitioners. Medical records protect continuity of care. Infection control protects the vulnerable. Procurement policies protect against fraud and expired medications. The field has learned repeatedly that good intentions do not substitute for systems.
Christians genuinely disagree about how much infrastructure is appropriate, especially when urgent needs press. Yet wise stewardship recognizes that avoidable medical errors, poor follow-up, and undisclosed conflicts of interest are not merely inefficiencies; they are failures of neighbor-love.
Training and local partnership can be a core program expense
Many Christian medical ministries invest in training local clinicians, strengthening hospital governance, and supporting community health networks. Those expenses can look like “indirect” work on paper, but they may produce the most durable patient impact over time. The When Helping Hurts framework, articulated by Steve Corbett and Brian Fikkert, has helped much of the Christian relief and development sector name why capacity-building often serves dignity better than perpetual dependence.

Fundraising and operating costs are morally relevant, not merely tactical
Donors often ask, with understandable concern, how much of a gift “goes to the cause” versus fundraising and administration. The harder question is what those categories actually represent. Fundraising can be exploitative or manipulative, but it can also be a truthful form of invitation into shared mission. Operations can be bloated, but they can also be the backbone of patient safety, legal compliance, and honest reporting.
The overhead debate changed, but the stewardship question did not
Much of the nonprofit sector has tried to correct simplistic overhead scorekeeping. Charity Navigator, Candid (formerly GuideStar), and the BBB Wise Giving Alliance jointly warned that overhead ratios are a misleading measure of nonprofit performance and can pressure organizations into underinvesting in systems that support results and accountability Charity Navigator.
That correction is necessary, but Christian donors should not misread it as permission to stop asking hard questions. Scripture commends careful stewardship; it does not commend vague reassurances. The aim is not to ignore costs, but to interpret them in light of mission clarity, truthful communication, and evidence of results.
Underfunding operations can create spiritual and organizational distortions
Nonprofits that feel forced to present themselves as “low overhead” may slide into fragile staffing, inadequate controls, and delayed maintenance that eventually raises costs and risks patient harm. Stanford Social Innovation Review described the “nonprofit starvation cycle,” in which pressure to minimize overhead leads organizations to underinvest in capacity, weakening performance and reinforcing donor skepticism Stanford Social Innovation Review.
Medical ministry magnifies those risks. Under-resourced compliance can expose patient data. Weak financial controls can invite fraud. Underpaid staff can lead to burnout and turnover that harms care continuity. Donors are right to care about cost discipline, and they should also care about whether a ministry is starving the very systems that protect patients and preserve integrity.
Fundraising methods reveal theology as much as they reveal strategy
How a ministry raises money is itself a form of discipleship. Appeals that trade in exaggeration, unverified miracle narratives, or guilt-driven manipulation contradict the God of truth. Appeals that speak plainly about needs, costs, and expected outcomes honor the donor as a steward and honor the beneficiary as a neighbor rather than a prop.
In our verification work at Most Trusted, we find that ministries meeting The Most Trusted Standard tend to treat fundraising as communication under moral constraint: claims are bounded, images are respectful, and donor intent is handled with seriousness rather than as a technicality.
Restricted gifts, designated funds, and the ethics of donor intent
Christian donors often want to designate gifts to a specific clinic, a particular country, a children’s program, or a shipment of medicines. Restrictions can be an expression of careful stewardship, and they can also create rigidity that weakens care. The ethical center is not whether restrictions exist, but whether the ministry solicits them honestly and administers them faithfully.
Healthy restriction practices begin with clarity before the gift
A ministry should explain what “restricted” means in practice: how funds are tracked, what happens if a project is fully funded, and whether the donor is granting discretion within a defined scope. The most common integrity failure in restrictions is not outright theft; it is ambiguity—language that implies specificity while reserving broad reassignment rights in fine print.
Donors should look for plain statements about whether a gift is legally restricted or merely designated for internal budgeting. Both can be appropriate, but they are different commitments.
Restrictions can unintentionally skew care priorities
Medical work has unglamorous necessities: sterilization supplies, generator maintenance, lab quality control, data systems, and salaries for local staff who provide year-round care long after a visiting team has left. If donor restrictions consistently favor visible items and episodic events, a ministry can become well-supplied in headlines and under-supplied in fundamentals.
A responsible ministry will sometimes push back gently on donor preferences, not to protect institutional comfort, but to protect patient welfare and long-term capacity. This is one place where governance maturity matters: leadership must have the courage to fund what is needed, not only what is marketable.
Accounting and reporting should make restricted funds auditable
When restricted gifts are significant, donors should expect to see evidence that funds are tracked and reported in ways that an auditor can test. This may show up in notes to financial statements, in separate fund reporting, or in clear program reports that connect expenditures to the restricted purpose. The point is not perfection in presentation; it is that a donor’s intent is treated as a trust before God.
What donors should examine when a ministry reports financial results
Financial statements can reveal far more than whether a ministry is solvent. They can reveal whether an organization is governed, whether its claims are tethered to reality, and whether it is willing to be seen. The best ministries do not treat transparency as a marketing posture. They treat it as accountability to the church and to the Lord whose name they bear.
Start with audited financials and a credible board
Where scale warrants it, an independent audit is a meaningful baseline. It does not certify excellence, but it does increase the cost of deception and strengthens internal discipline. Donors should also pay attention to whether the board is real: independent members, regular meetings, conflict-of-interest policies, and evidence that governance is more than a family enterprise.
For donors who want a structured way to assess these elements across ministries, our work at Most Trusted applies The Most Trusted Standard across faith commitments, financial integrity, governance practices, and transparency. That framework is designed for donors who want verification rather than vibes.
Read the story the numbers are telling, not only the ratios
Program percentages can be informative, but they are not self-interpreting. A sudden drop in program expense might reflect a one-time capital investment in a clinic. A surge in administrative cost might reflect building the compliance systems required for responsible growth. Conversely, consistently low administrative spending might signal chronic underinvestment and future risk.
Donors should look for consistency between narrative and financial reality. If a ministry presents itself as primarily clinical care but shows relatively little program expense tied to medical activity, that discrepancy deserves a question. If a ministry claims rapid expansion but shows no corresponding investments in staffing, systems, or partnerships, that also deserves a question.
Effectiveness is not always easy to measure, but it must be pursued
Medical outcomes can be difficult to aggregate across contexts, and not every meaningful result fits into a single metric. Still, donors should expect ministries to pursue measurable indicators appropriate to their work: patient volume, treatment adherence, maternal and child health benchmarks, referral completion, follow-up rates, and training outputs. Qualitative testimony has a place, but it is not a substitute for responsible measurement.
Transparency should also include limitations. A ministry that admits what it cannot yet measure, or where results are mixed, is often more trustworthy than a ministry that reports only uninterrupted success.
Giving with confidence requires both compassion and scrutiny
Christian medical ministries use donations to fund direct care, sustain the systems that make care safe, invite broader participation through fundraising, and remain accountable through governance and reporting. The faithful donor question is not whether every dollar produces an immediate, visible medical act, but whether the ministry’s spending reflects truthful stewardship, durable love of neighbor, and a willingness to be examined.
For donors assessing where to support medical work, the most practical next step is to compare a ministry’s claims to what its financials, governance practices, and reporting actually show—and to do so in the larger context of Christian Medical Ministries. Compassion without scrutiny can fund harm. Scrutiny without compassion can become cynicism. Christian stewardship requires both.



