
Trauma-informed care shapes orphan care ministries by forcing a sober re-evaluation of what love requires when a child’s history includes loss, disruption, or abuse. For Christian donors, the question is not whether compassion is biblical; Scripture is unequivocal about God’s concern for the fatherless and the vulnerable (Psalm 68:5). The harder question is whether our methods align with what we now know about how trauma affects children, and whether our generosity strengthens families rather than unintentionally weakening them.
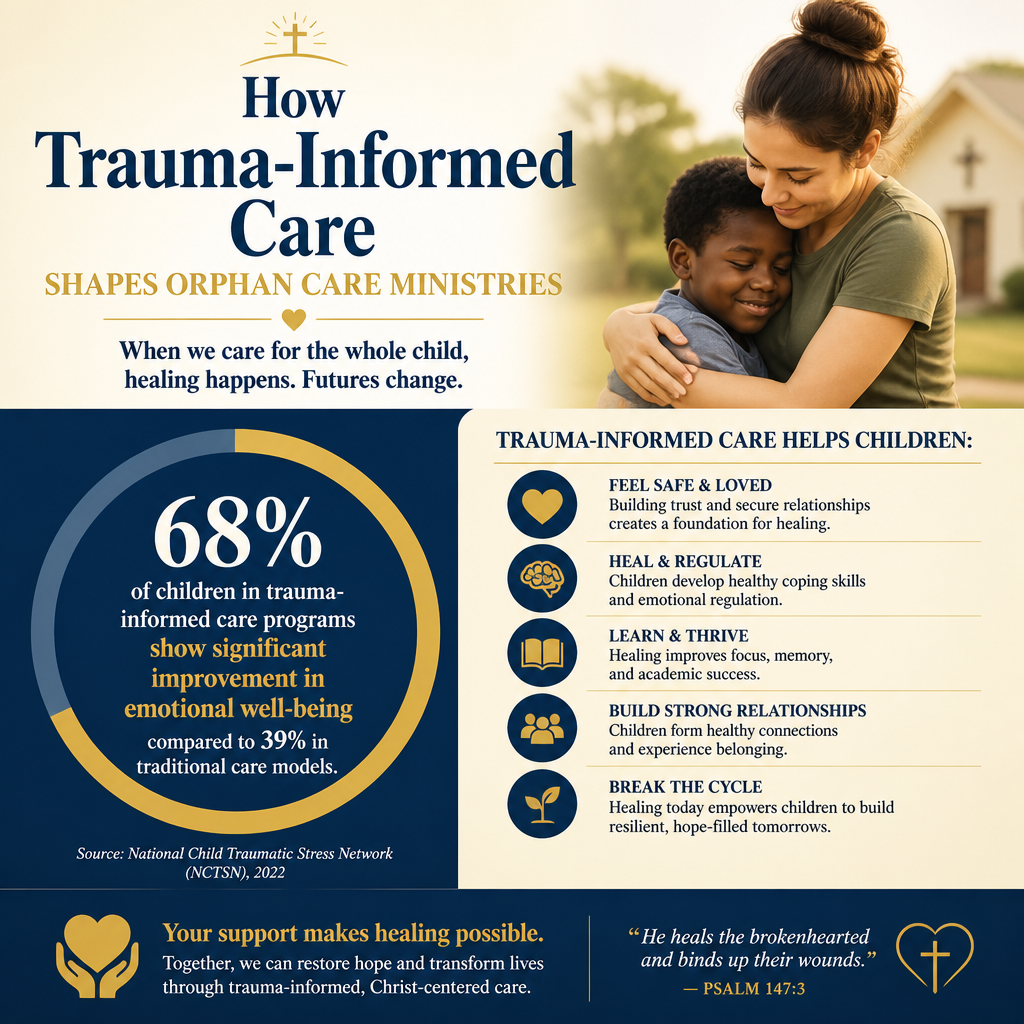
Orphan care work carries unique spiritual and emotional weight. It also carries unique risk. Children who have experienced separation from parents, repeated caregiver turnover, violence, or chronic neglect do not simply need a safe bed and a warm meal. They need relationships and environments that reduce threat, build secure attachment, and restore agency. Trauma-informed practice is not a trend imported from secular social work; it is, at its best, a disciplined application of neighbor-love that takes the human person seriously—body and soul, story and nervous system.
Trauma changes what children can receive from even good intentions
Behavior is often adaptation, not defiance
Trauma-informed care begins with a different interpretive lens. A child who hoards food, rejects affection, lies reflexively, or explodes in anger may not be “ungrateful” or “undisciplined.” Those patterns are often survival strategies learned in unsafe contexts. When ministries misread these responses as moral failure alone, they risk compounding shame and escalating control rather than building trust. Trauma-informed teams ask different questions: What happened to this child? What triggers threat responses? What helps the child return to a regulated state?
This is not permissiveness. Scripture affirms both compassion and moral formation. Yet wise formation requires knowing the student. Proverbs assumes that instruction is fitted to the person, not imposed as an abstraction. Trauma-informed practice makes that fitting more concrete by training caregivers to recognize hypervigilance, dissociation, or fight-flight-freeze responses, and to respond with calm, predictable structure rather than reactive power struggles.
Institutional settings intensify known risks
The modern orphan care movement has had to reckon with research showing significant developmental harm associated with institutionalization, especially for younger children. A widely cited review led by researchers affiliated with Harvard’s Center on the Developing Child describes how severe neglect and the absence of stable, responsive relationships disrupt brain development and stress-regulation systems in early childhood (Harvard University Center on the Developing Child). The point for donors is not to weaponize research against every residential program. It is to recognize that the most important “intervention” for a child is often the consistent presence of a nurturing caregiver.
What this means in practice is that ministries serious about trauma must either strengthen family-based care or, when residential care is unavoidable, design it to be as family-like and stable as possible—low caregiver turnover, consistent routines, and clear plans toward reunification, kinship placement, or adoption where appropriate.

Trauma-informed ministries re-center the family and the community
Orphan care is increasingly family preservation work
Christians genuinely disagree about the best models for caring for vulnerable children across cultures. Yet there is growing clarity about one central principle: many children labeled “orphans” have living family members, and poverty or crisis—not the absence of family love—often drives separation. UNICEF has repeatedly cautioned that the majority of children in institutions are not orphans and that family-based alternatives are generally preferable (UNICEF). Trauma-informed practice takes that reality seriously because unnecessary separation is itself a trauma.
This reframes what donors should be looking for. Strong orphan care ministries often devote significant capacity to preventing separation: emergency material assistance tied to a case plan, parenting support, counseling, domestic violence intervention partnerships, income stabilization, and connection to local churches. This is slower work, less photogenic work, and often more faithful work.
Reunification requires more than a transportation plan
When a child has been separated from family, reunification can be restorative, but it can also be destabilizing if handled carelessly. Trauma-informed ministries treat reunification as a clinical and pastoral process, not a logistics problem. That means careful assessment of safety, gradual transition, and ongoing follow-up support. It also means humility about what a ministry can control. A child’s healing depends on the integrity of the caregiving environment long after the ministry has reduced direct involvement.
For donors exploring the broader landscape of Orphan Care Ministries, this is one of the most important questions to ask: Does the ministry measure success primarily by how many children it houses, or by how many families it strengthens and how many safe, stable placements it supports over time?
Short-term missions can either reinforce attachment wounds or support long-term healing
Relational churn is not neutral
Many orphan care efforts are built around visiting teams. Done well, short-term trips can strengthen local staff, fund critical needs, and build prayerful solidarity. Done poorly, they can become relational churn for children who have already learned that adults arrive, attach, and disappear. Trauma-informed ministries set firmer boundaries: fewer “holding babies” experiences, less direct child bonding by visitors, and more support directed to consistent caregivers and family systems.
The field has had to grow up here. A 2017 UNICEF guidance document warned that volunteering in residential institutions can contribute to harm and recommended prioritizing family-based care and safeguarding standards (UNICEF). Donors can help by funding models that reduce dependency on rotating outsiders and increase investment in local staff capacity and oversight.
What donors can reasonably expect from healthy trip policies
Clear policies are not a sign of coldness. They are a sign that a ministry is serious about protecting children. Trauma-informed orphan care ministries typically communicate expectations before teams arrive and enforce them consistently, even when doing so disappoints visitors. Practices vary by context, but donors can look for a few common markers:
- Visitor-child interaction is structured, supervised, and designed to avoid exclusive bonding.
- Photos and stories are governed by child safeguarding and dignity standards, not marketing needs.
- Trips prioritize behind-the-scenes service, training, or community support rather than direct caregiving.
- Background checks and child protection training are required, not optional.
- Local leadership sets the agenda; visitors serve under local authority.
These disciplines align with Christian ethics of power. Jesus’s pattern is not extractive compassion; it is self-giving love that refuses to use vulnerable people to meet the emotional needs of the strong.
Trauma-informed practice should be visible in governance, staffing, and measurable outcomes
Training and supervision are spiritual and operational necessities
Trauma-informed care is often discussed as a frontline caregiving issue, but it is equally a leadership issue. If a ministry wants caregivers to respond with patience and skill, it must provide training, supervision, and manageable workloads. Chronic understaffing and constant turnover undermine even the best intentions. The result is predictable: more restraint, more punitive discipline, more crises, and more children labeled “difficult.”
This is where donors can bring needed realism. Residential and foster-care support models are labor-intensive. They require ongoing professional development, clear child protection protocols, and collaboration with local social services where possible. Ministries that treat “overhead” as a moral failing often end up with weak safeguarding and exhausted staff. The Overhead Myth statement—endorsed by Charity Navigator, GuideStar, and the BBB Wise Giving Alliance—argued that minimizing overhead is a poor proxy for impact (Charity Navigator). Trauma-informed work requires donors who understand that trained staff, supervision, and evaluation are part of caring well.
Evidence should include safety, stability, and permanency
Not every ministry can run a randomized controlled trial, and donors should not demand academic proof for every pastoral decision. But trauma-informed ministries do track indicators that correspond to child well-being. In orphan care, that typically includes placement stability, reunification rates with safety checks, school attendance and progress, and documented safeguarding incidents with transparent remediation. When a ministry reports only inputs—beds provided, meals served, visits hosted—it may be avoiding the more difficult question of whether children are experiencing durable healing.
Across our verification work at Most Trusted, ministries that meet The Most Trusted Standard tend to treat measurement and transparency as moral obligations rather than public relations tools. They make room for hard news, not only encouraging stories. They also show donors how decisions are made when cases are complex and no outcome is clean.
Donor diligence should include trauma competence and theological integrity
Good theology does not excuse poor practice
Christian donors often assume that clear doctrinal statements guarantee wise care. Doctrine matters. The Faith Foundation of a ministry shapes how it understands dignity, authority, and the image of God in a child. Yet trauma-informed care presses us to examine whether our practices reflect what we confess. A ministry can affirm orthodox theology and still operate with coercive control, weak safeguarding, or an unhealthy dependence on child separation to sustain fundraising narratives.
James’s command to care for orphans and widows is paired with a call to keep oneself “unstained from the world” (James 1:27). The biblical concern is not only that care happens, but that it happens with integrity. Trauma-informed practice, properly understood, is part of that integrity: it resists sentimentalism, refuses exploitation, and aims for restoration that respects the child’s whole person.
Questions that reveal whether trauma-informed commitments are real
Donors do not need to be clinicians to ask discerning questions. The ministries most prepared to serve traumatized children welcome scrutiny because it protects children and strengthens credibility. As donors consider How Orphan Care Ministries Serve Children and Families, a few questions reliably separate aspirational language from operational reality:
- What formal training do caregivers and supervisors receive in trauma and attachment, and how often is it refreshed?
- How does the ministry limit unnecessary child-caregiver disruption, including volunteer rotations?
- What is the ministry’s policy and track record on family preservation and reunification, including safety assessment?
- What child safeguarding standards govern reporting, investigation, and accountability?
- How does the ministry report outcomes that include stability and permanency, not only activity metrics?
These questions are not adversarial. They are a form of stewardship. Donors are not only funding programs; they are funding formative environments that will shape children’s capacity to trust, attach, learn, and worship for decades.
FAQs for How trauma-informed care shapes orphan care ministries
Is trauma-informed care compatible with Christian discipleship and discipline?
Yes, when it is practiced with theological clarity. Trauma-informed care does not deny moral agency or the need for formation. It insists that caregivers interpret behavior with wisdom and respond in ways that build safety and trust. Christian discipline aims at restoration, not control, and it is accountable to the dignity of the child as an image-bearer. Trauma-informed practice can strengthen discipleship by reducing shame-based reactions and increasing stable, patient care.
How can donors tell whether a ministry is using trauma-informed language as marketing?
Marketing tends to emphasize vocabulary; mature practice emphasizes systems. Donors can look for concrete indicators: staff training schedules, written safeguarding policies, limits on volunteer-child bonding, clear pathways to family preservation and reunification, and transparent reporting when incidents occur. Ministries serious about trauma also budget for supervision, mental health partnerships, and evaluation—costs that are often absent when “trauma-informed” is primarily a slogan.
A donor’s role in trauma-informed orphan care
Trauma-informed care shapes orphan care ministries by moving the center of gravity from rescuing children out of hardship to restoring children within safe, stable relationships whenever possible. That shift is consistent with Scripture’s concern for justice and mercy: the protection of the vulnerable, the restraint of power, and the pursuit of lasting peace rather than momentary relief. Donors who fund this kind of work should expect fewer simple stories, more careful safeguarding, and greater honesty about complexity. That is not a loss of faith. It is often what faithfulness looks like when the stakes are a child’s life.



