
When Christian recovery ministries should hire licensed clinicians is not a question of spiritual maturity versus secular expertise. It is a question of stewardship: how a ministry protects the vulnerable, tells the truth about what it does, and builds a care model that matches the complexity of addiction, trauma, and co-occurring mental illness.
Donors often feel a legitimate tension here. We give because we believe Christ heals, because we have seen redemption that no clinical protocol can manufacture. And we also know that untreated psychosis, severe withdrawal, active suicidality, and complex trauma can turn a well-intentioned discipleship setting into a dangerous place for a suffering person and a liability for the ministry that received them.
Addiction recovery is spiritual formation and it is also clinical risk
Christian ministries are called to shepherd souls and bodies
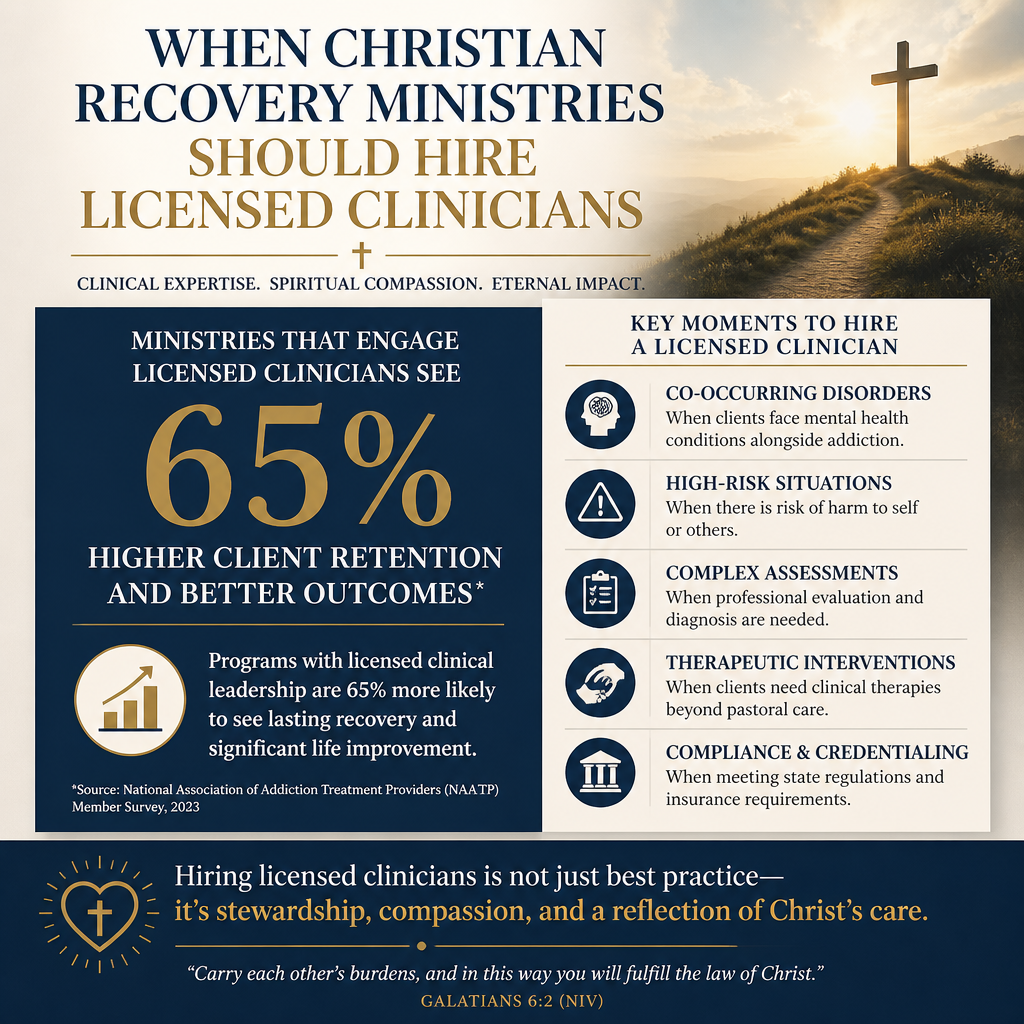
Scripture refuses the false divide between “spiritual” and “material.” The command to “bear one another’s burdens” (Galatians 6:2) is not an invitation to offer only words when a person’s body and mind are in crisis. Recovery ministry is often a front-door form of mercy: the church meeting people where they are, without preconditions, and walking with them toward repentance, repair, and renewed life.
At the same time, addiction is not merely a pattern of bad choices. It is frequently entangled with trauma histories, major depressive disorder, bipolar disorder, PTSD, and chronic medical conditions. The clinical literature consistently treats co-occurring disorders as common in substance use populations, which means that purely peer-led care can become overwhelmed by needs it was never designed to carry. SAMHSA frames integrated, coordinated approaches to co-occurring disorders as a best practice in treatment systems SAMHSA.
Withdrawal, suicidality, and psychosis are threshold questions
A ministry can love people sincerely and still be out of its depth when a participant presents with risk markers that require clinical assessment, documentation, and escalation protocols. This is not a fear-driven posture. It is the same logic by which churches install child safety policies: care for the flock includes limits, reporting, and competent protection.
Some ministries attempt to avoid “medicalization” by avoiding clinicians entirely, assuming that a more explicitly Christian environment will reduce risk. That assumption is not responsible. The National Institute on Drug Abuse describes addiction as a chronic, relapsing disorder involving changes in brain circuits related to reward, stress, and self-control National Institute on Drug Abuse. A biblical view of the person can hold this without surrendering moral agency or the need for repentance. It simply clarifies that some crises require licensed care, not only pastoral counsel.

When a ministry’s model crosses into clinical care
Licensure follows function, not mission language
Christian recovery ministries use a range of models: peer mentoring, residential discipleship, outpatient groups, recovery coaching, and partnerships with treatment providers. The question is not whether the ministry has a strong statement of faith. The question is what the ministry is functionally providing.
When a program begins diagnosing, treating, or managing mental health conditions; providing therapy; handling medication decisions; or conducting formal assessments that determine clinical placement, it is no longer only offering spiritual support. At that point, hiring licensed clinicians or formalizing a clinical partnership is often not optional if the ministry intends to operate with integrity and safety.
Common ministry scenarios that call for clinicians
Across our verification work at Most Trusted, we observe that confusion often arises when ministries grow beyond a small mentoring model into structured programming. Growth creates organizational pressure to “do more,” and the temptation is to make the program more intensive without adding the competencies that intensity requires.
- Residential settings where leaders manage crisis behavior, self-harm risk, or psychotic episodes
- Programs serving participants with histories of complex trauma, domestic violence, or sexual abuse
- Ministries accepting people directly from detox, incarceration, or emergency departments
- Any context where staff are expected to provide counseling that resembles psychotherapy
- Programs administering assessments that shape treatment planning or medication compliance
Christians genuinely disagree about the boundaries between pastoral counseling and clinical therapy. But donors should insist on clarity: what is pastoral care, what is peer support, and what is treatment. Confusion in this area usually harms participants first, then staff, and finally the credibility of the ministry’s public witness.
Clinical hiring is a governance decision before it is a staffing decision
Safety, liability, and reporting obligations require board-level oversight
When a ministry hires licensed clinicians, it is not merely adding a new “role.” It is changing risk categories, supervision requirements, documentation expectations, and often insurance coverage. The board must understand what clinical services are being offered, what the standard of care is in that jurisdiction, and how clinical oversight will function.
Many donors have seen ministries collapse after a preventable incident, followed by opaque communication and defensive posturing. The deeper issue is usually governance: no clear chain of responsibility, no written escalation protocols, and no independent review. The ministries that meet The Most Trusted Standard tend to treat participant safety as a matter of moral accountability, not merely legal exposure.
Clinical integrity protects the ministry’s spiritual mission
Some leaders fear that clinicians will displace prayer, Scripture, and discipleship. That fear is understandable if the ministry has experienced pressure to conform to secular norms. But clinical competence does not have to mean theological compromise. A clinician can serve under a doctrinal statement, respect pastoral authority in spiritual matters, and still insist on appropriate safety practices, evidence-based modalities, and referral boundaries.
What this means in practice is that donors should look for ministries that can articulate, in plain language, how clinical and pastoral leadership relate. Where does confidentiality apply and where do mandated reporting rules apply? Who can override a discharge decision? Who determines whether a participant is fit for a residential environment? These are not bureaucratic questions. They are questions of truthfulness and love of neighbor.
How donors can evaluate whether clinical staffing is warranted
Ask what populations the ministry serves and how intake works
Donors can ask direct questions without drifting into micromanagement. In well-governed ministries, leaders will not be offended by clarity. They will welcome it, because it forces the organization to name its actual model and its actual limits.
Start with intake. Does the ministry screen for severe mental illness, recent suicide attempts, or medical instability? Is there a written referral network for detox, inpatient psychiatry, domestic violence shelters, and trauma therapy? If the answer is “we take anyone and trust God,” the ministry may be confusing faith with presumption.
Look for verifiable boundaries and partnership pathways
Not every faithful recovery ministry needs clinicians on staff. Some programs can remain safely peer-led if they have disciplined boundaries and strong referral partnerships. The harder question is whether those boundaries are real or aspirational.
Healthy signs include written participation criteria, documented crisis protocols, and a pattern of referrals that is not treated as “failure.” A ministry that insists it can handle every case in-house is often a ministry headed for hidden harm.
Donors who want to compare programs across a landscape can situate these questions within the broader domain of Christian Addiction Recovery Ministries, where the range of models and risks varies substantially. The donor’s task is not to demand one model everywhere, but to fund ministries whose stated model matches their actual capacity.
Integrating clinicians without surrendering a Christian account of healing
Clinicians should strengthen discipleship, not replace it
Addiction recovery is not only cessation of substance use. It is rebuilding a life: truthful confession, repaired relationships, vocational stability, and spiritual endurance. Clinical care can address trauma symptoms, stabilize mood disorders, and teach skills for emotional regulation. Discipleship addresses worship, identity, repentance, reconciliation, and the reordering of loves. The two can be integrated without confusion when leadership insists on clear definitions.
In practice, clinicians can help ministries avoid spiritualizing mental illness, avoid shaming relapse in ways that increase secrecy, and implement trauma-informed practices that reduce re-traumatization. Trauma-informed care has become a widely adopted framework in behavioral health and social services, and SAMHSA’s guidance has shaped much of its common language SAMHSA. A ministry can adopt trauma-informed practices while remaining explicitly Christ-centered in its theological commitments.
Funding clinicians is a donor strategy, not just a line item
Some donors instinctively resist clinical hiring as “overhead.” That instinct deserves to be challenged. Proper clinical staffing can be a direct investment in outcomes and participant protection, especially in higher-risk models like residential programs. The Overhead Myth letter—signed by leaders including GuideStar and BBB Wise Giving Alliance—argues that simplistic overhead ratios mislead donors and can harm nonprofits by pushing them to underinvest in essential capacity BBB Wise Giving Alliance.
Across the work of Leadership and Operations in Christian Addiction Recovery, the strongest ministries are usually those that can describe, with specificity, what clinical capacity is necessary for their population, what is beyond their scope, and how they remain unambiguously Christian in mission and practice.
FAQs for When Christian recovery ministries should hire licensed clinicians
Does hiring clinicians mean a recovery ministry is becoming secular?
No. Hiring clinicians means the ministry is acknowledging the clinical risks present in its population and is choosing competent care as a form of love of neighbor. The determining issue is governance and clarity: whether clinicians serve within a Christian mission, whether pastoral discipleship remains central, and whether the ministry is transparent about what it does and does not provide.
Can a peer-led discipleship program be responsible without clinicians?
Yes, in some cases. Peer-led models can be responsible when they have disciplined boundaries, strong referral partnerships, documented crisis protocols, and leaders who do not confuse spiritual counsel with clinical treatment. As the population served becomes higher acuity, the case for licensed clinical oversight strengthens, and donors should expect the ministry’s model to evolve accordingly.
Stewardship requires matching care to complexity
When Christian recovery ministries should hire licensed clinicians is ultimately a question of truthful love. Ministries best honor Christ when they refuse both reductionisms: the reductionism that treats addiction as only a medical problem, and the reductionism that treats severe mental illness and withdrawal risk as issues discipleship alone can safely manage. Donors best serve the church’s witness when they fund ministries that name their scope, staff accordingly, and build systems that protect the vulnerable while proclaiming the hope of the gospel.



