
How Christian addiction recovery ministries measure impact is not a technical question for specialists; it is a stewardship question for donors. The church is rightly drawn to ministries that contend for men and women bound by substances, shame, broken relationships, and the spiritual despair that often accompanies them. But compassion does not remove the obligation to give truthfully, and measurable impact is one way we resist sentimental narratives that can mislead donors and harm participants.
For Christian donors, the heart of the matter is not whether a ministry can generate impressive numbers. It is whether the ministry can credibly show that people are being served with dignity, that claims match reality, and that the work reflects the character of Christ—especially when outcomes are slow, uneven, and costly. Across Christian Addiction Recovery Ministries, the strongest organizations treat measurement as part of discipleship and accountability, not as marketing.
Impact begins with a sound definition of what the ministry exists to produce
Addiction recovery is a contested space even before measurement begins. Christians genuinely disagree about the language of “recovery,” the role of medication-assisted treatment, and whether “sobriety” is the primary outcome or one fruit among many of repentance, reconciliation, and renewed life. A ministry cannot measure impact well if it has not defined what faithfulness looks like in its own model of care.
In practice, credible ministries separate three layers of results: activities (what they do), outputs (who they serve and what participants receive), and outcomes (what changes). Donors are often shown activities—classes offered, mentors trained, beds filled—because they are easy to count. Outcomes are harder and more spiritually weighty: sustained abstinence, reduced relapse severity, stable employment, restored family relationships, church connection, and growth in spiritual practices that endure when support is removed.
Faithful outcomes are broader than a single number
“Days sober” can matter, but it can also distort. A person may achieve abstinence while remaining isolated, unemployed, and estranged from family; another may experience a relapse after months of stability yet return quickly to treatment, confession, and support, with less harm than before. Ministries that measure well acknowledge that addiction is often chronic and relapsing, and they track indicators that reflect resilience, accountability, and community—markers that align with a Christian anthropology that sees human beings as embodied souls, not only behavior patterns.
Programs differ, so comparisons must be careful
A residential program serving people coming directly from homelessness and incarceration will likely show different short-term outcomes than an outpatient counseling ministry serving employed participants with strong family support. Donors should resist comparing ministries without attending to who is being served and what level of risk participants bring at intake. Measurement that ignores starting conditions rewards ministries that select easier cases and punishes those that serve the most vulnerable.
A ministry’s theology should shape its measurement
Scripture does not reduce transformation to a metric, yet it does insist on truthfulness, integrity, and fruit that can be observed over time. Jesus warned against public displays meant to be seen by others, and he also taught that “a healthy tree bears good fruit” (Matthew 7:17). Mature measurement aims for that posture: neither performative nor evasive, willing to describe fruit honestly, including where growth is incomplete.

Better measurement distinguishes between what can be counted and what must be discerned
Addiction recovery ministries often operate at the intersection of clinical realities and pastoral care. That complexity is not a reason to avoid evidence; it is a reason to use evidence wisely. The most credible ministries measure what is measurable, but they do not pretend that every meaningful change can be reduced to a spreadsheet.
Use validated tools where they fit
When ministries claim improvements in mental health, substance use severity, or functioning, the strongest ones use established screening and outcome instruments administered consistently. Donors need not become clinicians, but it is reasonable to ask whether outcomes are based on standardized assessments, on self-report without structure, or on staff impressions. Where a ministry partners with licensed providers, measurement may include clinically recognized indicators; where it operates primarily as a discipleship community, measurement may focus more on retention, community engagement, and long-term stability.
Track intermediate outcomes, not only final outcomes
One of the common failures in donor reporting is a fixation on a single “success rate.” In addiction care, the harder truth is that intermediate outcomes often predict long-term stability: consistent attendance, completion of core programming, active participation in peer support, reunification steps with family, compliance with probation where relevant, and regular involvement in a local church. These do not replace long-term outcomes, but they provide a more honest picture of whether the ministry is building durable habits rather than chasing a headline.
Honor the limits of attribution
Ministries should be careful about claiming that they “caused” a person’s transformation. Human change involves agency, grace, relationships, and often multiple interventions over time. The question for donors is not whether the ministry claims sole credit, but whether it can credibly show that its program contributes to measurable improvements and that participants are safer, more stable, and more spiritually grounded because of the ministry’s involvement.
Transparent ministries report outcomes with safeguards that protect people and strengthen trust
In addiction recovery, privacy is not a secondary concern. Improper disclosure can cost someone employment, housing, custody arrangements, or personal safety. It can also violate law and professional ethics for ministries that handle protected health information. Donors should treat strong privacy practices as a sign of seriousness, not secrecy.
Protect client privacy without hiding performance
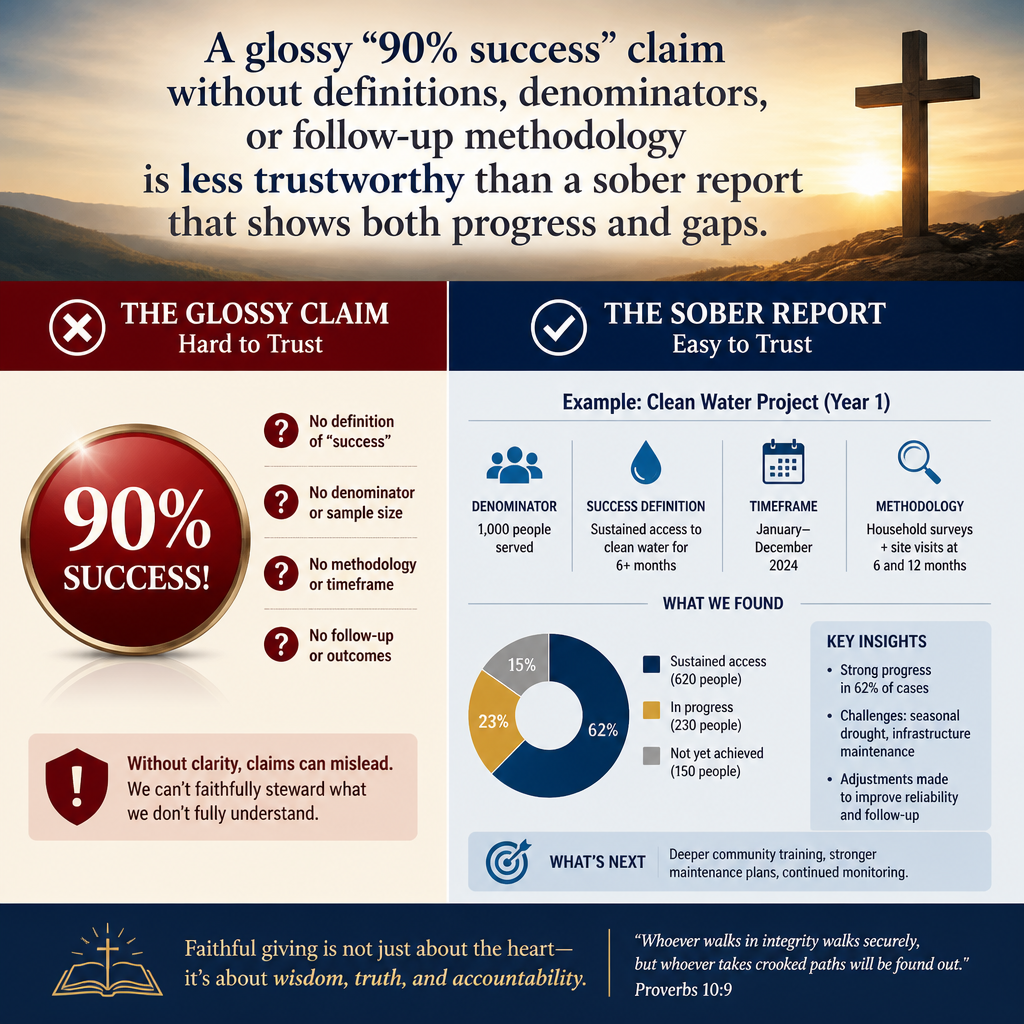
Outcomes can be reported in aggregate, with clear definitions and time windows, without exposing identifiable details. Ministries that do this well explain their data collection methods, their follow-up rates, and how they handle participants they cannot reach. A glossy “90% success” claim without definitions, denominators, or follow-up methodology is less trustworthy than a sober report that shows both progress and gaps.
Where ministries operate in the United States and handle health information through covered entities or formal clinical partnerships, donors should expect awareness of HIPAA expectations and secure data handling practices. HIPAA’s official resources are clear that protected health information requires specific safeguards and limits on disclosure U.S. Department of Health and Human Services.
Use stories with informed consent and pastoral restraint
Impact stories have a rightful place in Christian giving because they bear witness to God’s mercy in real lives. They also carry risk. A story can pressure a participant to perform gratitude, disclose more than is wise, or become a public example before their stability is established. Mature ministries obtain informed consent, avoid coercive incentives, and offer the option to share anonymously or to withhold details that could identify family members or legal circumstances.
Donors can ask a simple, telling question: “What is your process for consent, and who is protecting the participant’s interests when a story is told?” Ministries that answer with clarity tend to be ministries that have confronted real ethical dilemmas rather than assuming good intentions are enough.
Report with humility about relapse and complexity
A ministry that never mentions relapse may be omitting reality. Research and clinical experience recognize relapse as a common feature of substance use disorders, and a responsible program prepares for it through aftercare, mentoring, and rapid re-engagement. Donor reporting should not normalize relapse as inevitable, but it should acknowledge it as a risk and demonstrate what safeguards exist to reduce harm when relapse occurs.
Donors should look for measurement that is governed, audited, and spiritually coherent
Measurement quality is not only a program question; it is a governance question. Data can be manipulated under pressure, and staff can be incentivized to present outcomes that secure funding rather than reflect truth. The ministries most worthy of long-term donor partnership are those with structures that reward accuracy, protect participants, and resist the temptation to trade integrity for growth.
Board oversight and leadership accountability
Healthy ministries can explain who reviews outcome reports, how often leadership examines them, and what actions follow. If data never influences decisions—staffing, program design, aftercare strategy—then measurement may be a donor artifact rather than an internal discipline. Conversely, when boards ask hard questions about retention, safety incidents, and long-term stability, ministries are more likely to improve without drifting from their mission.
Financial integrity supports truthful reporting
Donors often separate “program impact” from “financial stewardship,” but the two are linked. A ministry with weak financial controls is more vulnerable to exaggerated claims and to hidden crises that harm participants. Independent financial review—whether a full audit or another appropriate level of external scrutiny—does not prove impact, but it strengthens credibility and reduces the likelihood that donors are funding an unstable operation. For context on the role of audited financial statements in nonprofit accountability, the National Council of Nonprofits outlines common practices and expectations National Council of Nonprofits.
Effectiveness is not the same as efficiency
Christian donors rightly want resources used well, but addiction recovery rarely fits a low-cost model. Trauma-informed care, trained staff, secure facilities, and sustained aftercare require real expense. The widely endorsed “Overhead Myth” letter—signed by leading nonprofit information organizations—warns donors against using simplistic overhead ratios as a proxy for effectiveness Candid GuideStar. In recovery ministry, the better question is whether spending aligns with the ministry’s theory of care, whether financial reporting is clear, and whether outcomes justify continued investment.
Giving with confidence requires impact evidence that can bear the weight of trust
Christian addiction recovery ministries measure impact well when they define outcomes with theological clarity, use appropriate tools without pretending to control every variable, report results with privacy safeguards, and submit their claims to governance and financial accountability. Donors should not demand perfection from ministries serving people in crisis, but we should expect integrity, candor, and evidence that the work is producing fruit that endures. At Most Trusted, our verification work applies The Most Trusted Standard so donors can distinguish between compelling stories and credible stewardship, and partner with ministries whose impact claims are worthy of the trust they seek.



