
Funding care access in Christian counseling is not primarily a question of generosity; it is a question of whether the church will bear one another’s burdens in a way that is clinically responsible and spiritually faithful. Donors often sense the tension immediately: counseling is expensive, need is widespread, and the outcomes are personal and hard to measure without reducing people to metrics.
Scripture does not treat suffering as an abstraction. Elijah despaired (1 Kings 19). David’s prayers carry anguish without embarrassment. Jesus met people in distress with truth and mercy, never confusing compassion with sentimentality. Christian counseling ministries stand in that tradition when they provide care that is both pastorally grounded and clinically competent—and when they build funding models that make that care accessible to those who cannot pay market rates.
Why access is the central funding question
Christian donors are accustomed to funding tangible needs: meals served, shelters built, Bibles distributed. Counseling is different. The “need” is often invisible, the path to healing is rarely linear, and the cost structure is shaped by licensed labor and clinical standards. When we fund access, we are not buying a commodity; we are underwriting the slow, attentive work of presence, assessment, and skillful care.
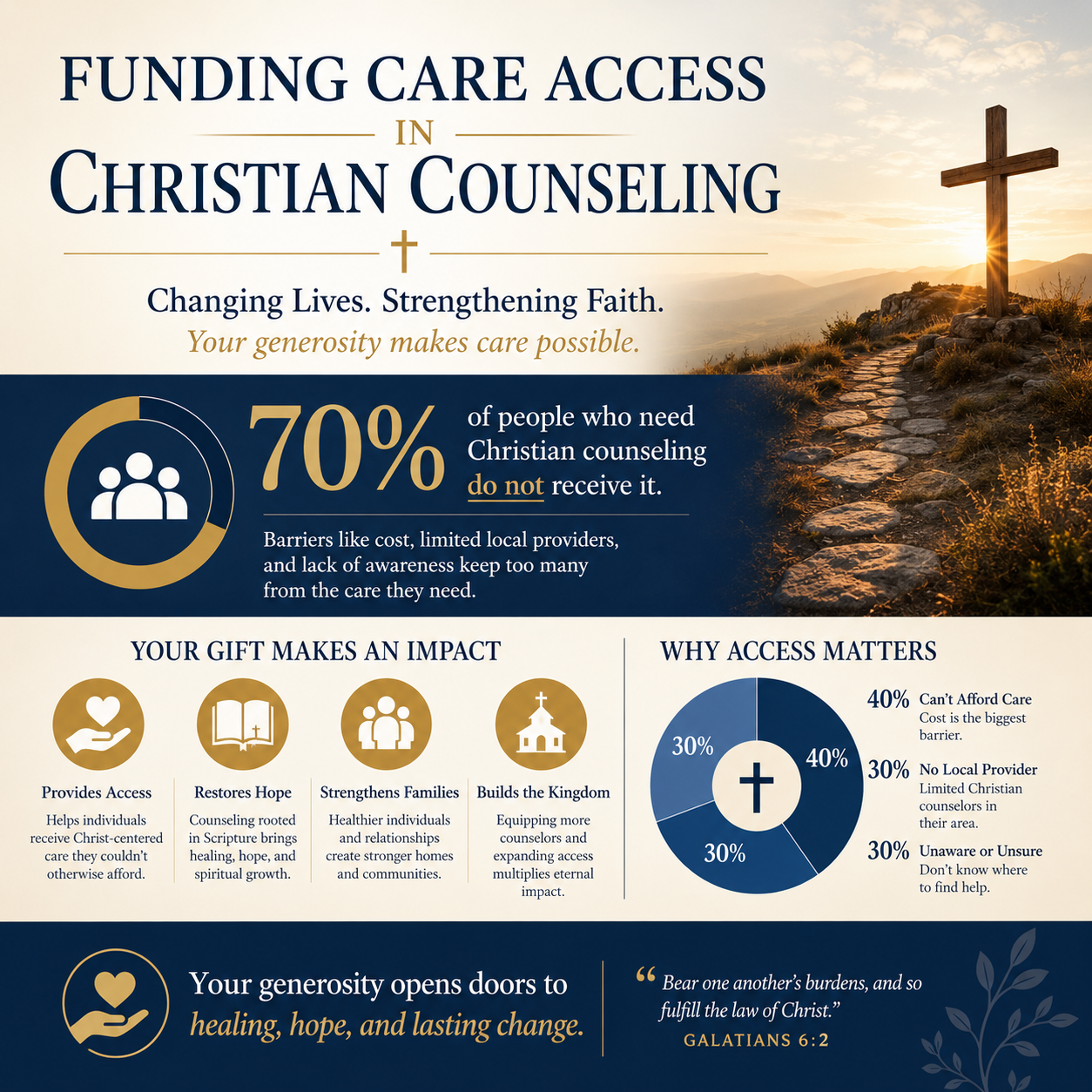
The national mental health workforce shortage is not speculative. Federal health agencies continue to describe persistent gaps in access, especially in rural and underserved areas, which has direct implications for waitlists and referral patterns in Christian counseling settings. The Health Resources and Services Administration maintains ongoing designation data on shortage areas through its Health Workforce Shortage Areas program at HRSA.
What this means in practice is that many ministries face two simultaneous pressures: (1) demand that outstrips clinical capacity, and (2) pricing that must honor the real cost of qualified counselors while not excluding lower-income clients. Donors sometimes attempt to solve this by insisting on very low fees across the board. That instinct can unintentionally push ministries into the starvation cycle described by Ann Goggins Gregory and Don Howard, in which chronic underfunding erodes quality and effectiveness over time, as articulated in Stanford Social Innovation Review at SSIR.
In our work at Most Trusted, we see access initiatives succeed when leaders tell the truth about costs, build disciplined boundaries around clinical quality, and invite donors into a stewardship relationship rather than a rescue narrative.

How ministries actually reduce financial barriers
Not every “scholarship” model is the same. The best ministries choose an access strategy that matches their theology of care, their clinical model, and their local context. Donors serve those ministries well by asking for specificity: who is being served, how eligibility is determined, and how subsidy levels are set.
Sliding-scale counseling done with integrity
Sliding-scale counseling can be a faithful expression of shared burden-bearing, but only if it is administered with clarity and consistency. Ministries typically base fees on household income, number of dependents, and in some cases extraordinary expenses. The crucial safeguard is that the scale must be matched to a sustainable budget. If the “discounted” fee becomes the de facto norm, the ministry is forced to reduce supervision, shorten sessions, or overload counselors—each of which harms clients.
Donors can support sliding-scale models most effectively by funding the delta between the reduced fee and the true cost per session, not by pressuring the ministry to pretend the cost is lower than it is. This is where transparent unit economics matter: what does a session cost once clinical supervision, administrative support, facility expenses, training, and compliance requirements are properly included?
Sponsoring counseling and the dignity of the client
Many ministries invite donors to “sponsor” counseling for a client or a set number of sessions. Done well, this is not a one-to-one patronage arrangement; it is a pooled fund that protects privacy and avoids subtle coercion. Theologically, it aligns with the pattern of the early church’s shared provision, where resources were distributed according to need without turning need into a spectacle.
Donors should expect ministries to guard confidentiality rigorously, including appropriate HIPAA practices when applicable and clear internal policies that prevent donor influence over clinical decisions. A ministry that offers moving stories but cannot explain how it protects client dignity is asking donors to fund risk.
Scholarship funds and the reality of complex cases
Scholarship funds are often necessary because the highest-need clients typically require more sessions, more coordination, and sometimes more specialized clinicians. Trauma, addiction, severe anxiety, and comorbid conditions can demand longer treatment horizons. If scholarships are capped at a token amount, access becomes symbolic rather than real.
At the same time, donors should not assume that “more sessions” automatically means “better ministry.” Good clinical care includes appropriate discharge planning, measured goals, and referrals when a client’s needs exceed the ministry’s scope. The harder question is whether scholarship funds are governed by a clinical and ethical framework rather than by donor preference or the ministry’s desire to report large numbers served.
Waitlists, referrals, and the obligation to practice within limits
Reducing waitlists is one of the most common donor aspirations in this field, and it is usually a worthy one. Yet a shorter waitlist achieved by lowering intake standards or rushing assessments can place vulnerable people at greater risk. Christian compassion does not excuse clinical negligence.
Capacity is more than headcount
Adding counselors can help, but capacity is also shaped by supervision, documentation, scheduling infrastructure, and policies for crisis escalation. Many ministries rely on a mix of licensed clinicians, supervised interns, and pastoral care staff. That blend can be appropriate, but donors should ask how roles are defined and how supervision is funded. Intern-heavy models without strong oversight can create uneven quality and ethical exposure.
Some ministries build group counseling, psychoeducation cohorts, or skills-based classes as a front door to care. For certain conditions, group formats can be clinically appropriate and financially efficient. But the ministry should be able to name which populations they serve well in group settings and which require individualized care.
Referral networks are not a sign of failure
Christian counseling ministries should refer to clinical care outside their walls when acuity is high, when medication management is needed, or when specialized treatment is required. Donors sometimes interpret referrals as a lack of faith or a lack of competence. In reality, a mature ministry knows its limits and prioritizes client safety.
Wise donors ask about referral pathways: relationships with psychiatrists, inpatient facilities, domestic violence resources, substance use treatment, and emergency services. A ministry that cannot describe its crisis protocol is not ready to scale access.
Serving the most vulnerable without creating dependency
Christians genuinely disagree about the right balance between subsidizing care and encouraging personal responsibility. The concern is not theoretical. Long-term subsidy without clear goals can foster dependency; aggressive cost-sharing can exclude the poor. The When Helping Hurts framework, articulated by Steve Corbett and Brian Fikkert, has shaped donor thinking by emphasizing dignity, agency, and the difference between relief, rehabilitation, and development; see the authors’ work through Chalmers Center.
In counseling, this often translates into time-limited scholarship plans paired with clear clinical objectives and periodic review. It can also include practical supports that strengthen stability—job coaching referrals, budgeting help, pastoral discipleship, or community-based supports—without confusing counseling with a catch-all solution.
What donors should verify before funding access
Funding care access is spiritually meaningful, but it is also operationally complex. The donor’s calling is not to become a clinician; it is to practice informed stewardship. That stewardship improves when donors insist on evidence of faithfulness and competence, not just good intentions.
Most Trusted exists to help donors give with confidence by evaluating ministries against The Most Trusted Standard, a 15-criteria framework that examines faith foundation, financial integrity, governance and leadership, and transparency and effectiveness. Those categories matter in counseling because the stakes are high: mishandled care can deepen harm, expose clients, and discredit Christian witness.
Governance that protects clinical independence
Donors should look for boards that understand the difference between spiritual oversight and clinical micromanagement. A strong board asks whether the ministry has licensed leadership where needed, appropriate policies, and a culture that takes ethical constraints seriously. Clinical independence matters because counselors must be free to recommend what is clinically appropriate, even when it is costly or inconvenient.
Red flags include donor-driven promises about outcomes, pressure to share identifiable stories, or spiritualized language used to dismiss evidence-based practice. A ministry can be explicitly Christian and still operate with clinical rigor; donors do not need to choose between theological conviction and professional competence.
Financial integrity that tells the truth about cost
Access work collapses when ministries hide the true cost of care. Donors should expect budgets that distinguish between program expense and the real infrastructure required for safe counseling: training, supervision, compliance, and secure record systems. The nonprofit sector has repeatedly warned against simplistic “overhead” policing; the Overhead Myth letter, signed by leaders including Charity Navigator and BBB Wise Giving Alliance, remains a key reference point for why administrative investment can be necessary for impact, available through Charity Navigator.
A ministry’s access strategy should be visible in its financial model. If a counseling center advertises broad scholarships but shows no designated revenue stream, donor-funded access may be functioning as an unfunded mandate placed on clinicians.
Transparency and effectiveness without reducing people to numbers
Counseling outcomes are difficult to summarize publicly, and confidentiality limits what should be shared. Still, donors can reasonably ask how ministries assess progress and maintain quality. Many responsible centers use validated clinical instruments (for example, symptom or functioning measures) alongside qualitative review and supervision. The question is not whether the ministry can promise a cure, but whether it can demonstrate disciplined care: appropriate intake, treatment planning, documentation, and follow-up.
We also look for clarity about who is being served. Some ministries focus on pastors and ministry leaders, others on couples, children, trauma survivors, or low-income communities. Donors should not assume a single “most biblical” target population; the responsible question is whether the stated mission aligns with the actual client mix and whether access funding is reaching the intended people.
For readers assessing counseling ministries within a broader giving portfolio, our coverage of Christian Counseling Ministries addresses common models, risks, and verification considerations that shape trustworthy funding decisions.
Funding access as a form of faithful stewardship
Funding care access in Christian counseling is an investment in patient, often unseen mercy. The most trustworthy ministries neither romanticize suffering nor monetize it; they tell the truth about cost, protect clients, and practice within ethical limits. Donors serve this work best by underwriting sustainable access—so that compassion does not depend on crisis fundraising, and so that those who seek help are met with competent care and Christian hope in the same room.



