
What volunteer roles pregnancy resource centers need most is not only a staffing question; it is a theological question about how a community embodies truth and mercy at the same time. A mature pregnancy resource center is not simply offering a “service.” It is receiving a neighbor in crisis and practicing a form of ministry that requires spiritual clarity, emotional steadiness, and operational competence.
For Christian donors, volunteer capacity is also a leading indicator of organizational health. A center can have a compelling mission statement and a moving testimonial, yet still lack the disciplined systems that protect clients, safeguard funds, and ensure that compassion does not become coercion or carelessness. Across our verification work at Most Trusted, we see that ministries that meet The Most Trusted Standard tend to treat volunteer roles as governed responsibilities, not informal enthusiasm.
Why the most needed roles are often the least visible
Pregnancy resource centers are sometimes evaluated in public conversation as if their only meaningful outputs are diapers, ultrasounds, and counseling sessions. But the work that makes those services ethically and spiritually credible is frequently hidden: training, documentation, supervision, confidentiality, and referral discipline. Those “back-of-house” tasks are rarely what volunteers imagine when they first inquire, which is precisely why they become chronic shortages.
The New Testament’s description of the church includes both public ministry and ordered administration. Acts 6 portrays a moment when the apostles refuse to let food distribution become neglected, and the solution is not guilt but structure: qualified people are appointed so that the ministry of the Word and the ministry of mercy can both be carried faithfully. Pregnancy resource centers, at their best, are living out that same refusal to choose between care and order.
Volunteer need is shaped by compliance, not only compassion
Centers operate under real constraints: HIPAA-adjacent confidentiality expectations, mandatory reporting requirements that vary by state, medical director oversight where medical services are provided, and donor restrictions on certain funds. Volunteers who can reliably work within these constraints are unusually valuable because they protect clients from harm and protect the ministry from preventable crisis.
The donor question behind volunteer roles
Donors often ask whether a center is “using volunteers well.” The harder question is whether the center has defined roles that reduce risk, set clear boundaries, and make faithful outcomes more likely. When volunteer work is poorly governed, the center may drift toward what the When Helping Hurts framework, articulated by Steve Corbett and Brian Fikkert, warns against: assistance that unintentionally weakens dignity, agency, and long-term resilience.

Frontline client care roles that require the strongest formation
Not every volunteer is suited for direct client work, and wise centers say so plainly. The most needed frontline roles are those that combine empathy with disciplined communication. Clients are often navigating fear, relational instability, economic pressure, and complicated moral terrain. A volunteer who can remain present without becoming directive is not easily replaced.
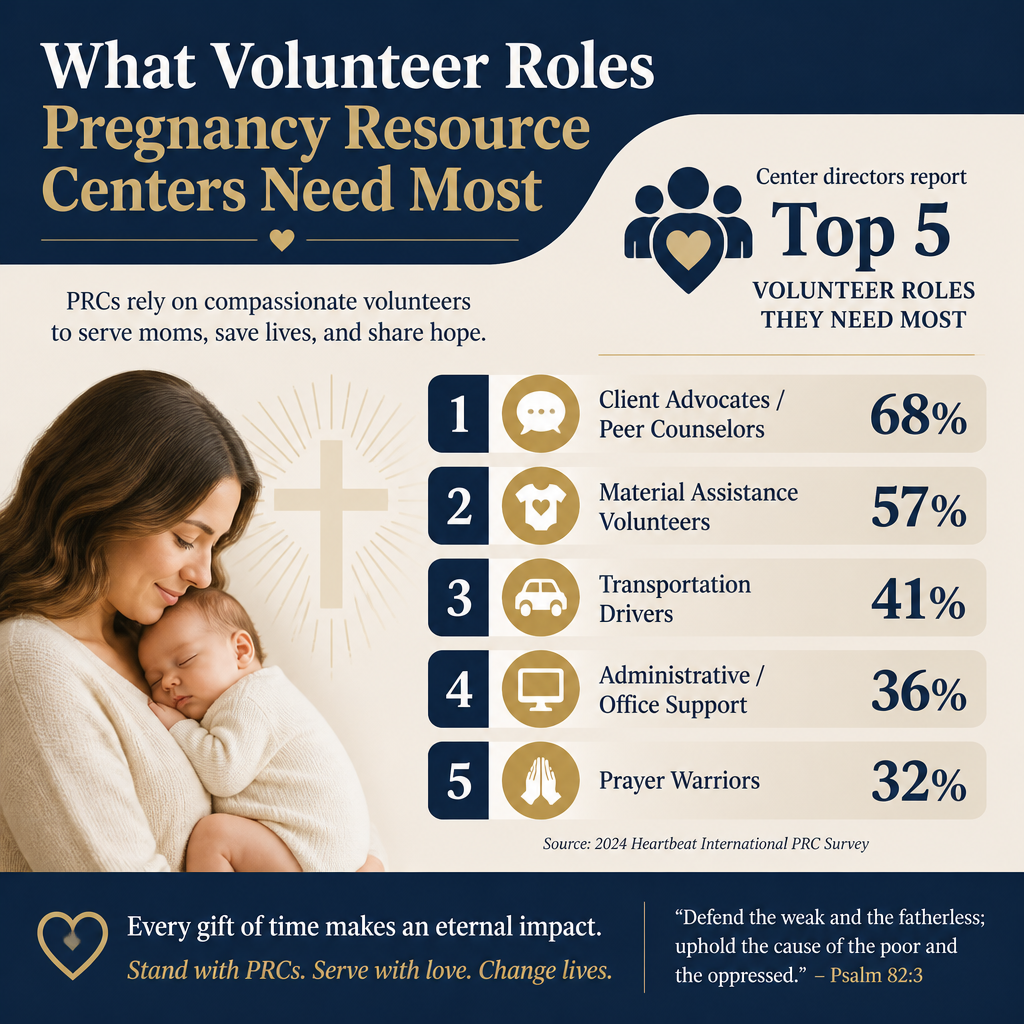
Client advocates and peer counselors
In many centers, client advocates are the relational core of the ministry: they welcome clients, conduct intake, explain services, and provide ongoing coaching through parenting education or life skills curricula. These roles demand consistent training in trauma-informed care, boundaries, and documentation. They also require theological steadiness: the capacity to speak truthfully about human dignity without turning a person into an argument.
Centers that are transparent about training requirements and supervision tend to be healthier over time. Donors should not interpret this as bureaucracy; it is a form of pastoral prudence applied to vulnerable circumstances.
Ultrasound and medical support volunteers where appropriate
Some centers provide limited medical services, including ultrasound. Where that is the case, licensed medical volunteers and support staff can be among the most critical needs. The standard here is not enthusiasm but credentialed competence and proper oversight. Donors should expect the center to be clear about medical governance, professional supervision, and the limits of what is offered.
Because medical services carry heightened regulatory and liability exposure, strong centers tend to be more selective, not less, about volunteer onboarding. That selectivity is often a marker of seriousness.
Aftercare and material support roles that reduce repeat crisis
Pregnancy resource centers sometimes become known for a first appointment. The more enduring work is what follows: parenting support, community referrals, and practical assistance that stabilizes a family over months rather than minutes. Volunteers who can persist over time, without saviorism and without fatigue-driven withdrawal, are frequently the difference between episodic help and sustained care.
Parenting education and mentoring
Many centers run parenting classes, mentorship programs, or “earn while you learn” style education paired with material resources. These programs can be deeply constructive when they are not treated as a transactional exchange. Volunteers in these roles need to understand adult learning, poverty dynamics, and the ethical line between encouragement and manipulation.
Donors should ask how participation is framed and whether the center tracks outcomes beyond attendance. A center can offer classes and still fail to measure whether clients are gaining skills, accessing appropriate healthcare, or moving toward stable housing and employment supports.
Material resource coordination and compassionate logistics
Diapers, car seats, baby clothing, and formula distribution require operational discipline: inventory controls, fair eligibility guidelines, and clear communication. Volunteers who can organize, sort, schedule pickups, and maintain dignified distribution systems are often more needed than people realize.
- Inventory intake and categorization with basic controls
- Appointment-based distribution to reduce chaos and protect privacy
- Quality and safety checks for car seats and cribs
- Donation receipt documentation aligned with accounting practices
- Client follow-up scheduling tied to education or care plans
These tasks can feel mundane, but they are where a ministry’s respect for clients becomes tangible. When distribution becomes disorganized, clients experience it as disregard, even if the intentions were generous.
Operational and governance roles that donors should prize
Some of the most strategic volunteer roles are not public-facing at all. They are roles that strengthen financial integrity, governance, and transparency. Mature donors often focus on whether a ministry has “low overhead,” but the Overhead Myth letter signed by Charity Navigator, Candid, and BBB Wise Giving Alliance argues that overhead ratios are a poor proxy for effectiveness and can even pressure nonprofits into unhealthy underinvestment in infrastructure Charity Navigator.
Pregnancy resource centers are no different. Under-resourced administration can result in weak controls, poor recordkeeping, and preventable reputational damage. Donors should prize volunteers who help a center become more accountable.
Finance support, data hygiene, and donor stewardship
Not every center can afford robust back-office staffing, especially in smaller communities. Skilled volunteers can help with bookkeeping support under appropriate supervision, database management, donation acknowledgments, and basic reconciliation tasks. The key is proper separation of duties and clear oversight. A volunteer should not be a single point of failure for financial controls.
Across our verification work, we find that donor trust rises when ministries can produce clear, timely, consistent reporting. For donors who want to give with confidence, this is not cosmetic. It is part of the ethical duty to “take pains to do what is right, not only in the eyes of the Lord but also in the eyes of man” (2 Corinthians 8:21).
Board-adjacent expertise without board capture
Some volunteers can strengthen governance through policy review, risk management, HR counsel, or legal guidance. The tension is real: board-adjacent volunteers can also become informal power centers if authority is unclear. Well-governed centers define decision rights, maintain written policies, and refuse to outsource accountability.
This is one place where donors can gently press for maturity. A center can be doctrinally faithful and still be operationally fragile. The Most Trusted Standard treats governance and transparency as spiritual responsibilities, not merely nonprofit best practice.
Church and community roles that extend the center without politicizing it
Pregnancy resource centers operate within a contested public narrative. Christians genuinely disagree about messaging strategy, policy engagement, and public advocacy. Some donors want louder public witness; others want quiet excellence. What this means in practice is that volunteer roles that strengthen the center’s relational credibility can be as important as roles that increase volume.
When a center becomes defined primarily by what it opposes, it can unintentionally narrow the very network of care that makes long-term support possible. When it avoids moral clarity, it can lose its reason for being. The needed volunteer roles are those that help the center remain both truth-speaking and serviceable to real neighbors.
Church liaison and pastoral integration
Many centers need volunteers who can serve as thoughtful liaisons to local churches: coordinating baby showers, recruiting volunteers for specific shifts, arranging prayer support, and educating congregations on what the center does and does not do. This role requires maturity, because it involves setting expectations. Not every church partnership is automatically healthy; some become transactional or overly controlling.
For donors who want a wider view of the field, we track patterns and concerns across Pregnancy Resource Centers with an emphasis on verifiable practices rather than marketing claims.
Community referral coordination
Centers are rarely equipped to address every downstream need: housing instability, domestic violence, substance use disorder, immigration legal services, or specialized mental health care. Volunteers who can build and maintain a vetted referral network help a center avoid overpromising and underdelivering.
Referral discipline is also an integrity issue. A center that makes referrals without due diligence can inadvertently send a client into harm. Donors should ask how partners are vetted and whether the center documents referral outcomes.
FAQs for What volunteer roles pregnancy resource centers need most
Which volunteer roles should donors be most eager to fund or underwrite?
Donors often gravitate toward visible services, but the highest-leverage roles are frequently training, supervision, data integrity, and follow-up systems. Underwriting volunteer training curricula, background checks, secure data systems, and staff oversight strengthens the entire ministry. These investments align with the “pains to do what is right” ethic in 2 Corinthians 8 and tend to reduce the risk of preventable failures.
How can donors tell whether a center uses volunteers responsibly?
Responsible centers define roles in writing, require appropriate screening and training, maintain confidentiality practices, and supervise volunteers with consistent documentation. They also show humility about limitations, especially around medical services and complex social needs. For donors comparing ministries, our work at Most Trusted applies The Most Trusted Standard so that questions of governance, financial integrity, and effectiveness are evaluated with evidence rather than assumption, including within Volunteering at Pregnancy Resource Centers.
Donor discernment and the roles that sustain faithful presence
The volunteer roles pregnancy resource centers need most are those that make compassion durable: trained client advocates, competent medical support where applicable, organized aftercare, and the administrative disciplines that protect both clients and the witness of the church. Donors serve these ministries best by valuing what is quiet and structural as much as what is visible and immediate.



