
What training pregnancy resource centers require for volunteers is not a minor operational detail. It is one of the clearest indicators of whether a center understands its work as both mercy and moral responsibility, especially when vulnerable clients are making time-sensitive decisions under pressure.
For Christian donors, volunteer training is also a stewardship question. Many supporters give because they want women and families met with compassion, truthfulness, and competent care. When training is thin, the risks are predictable: spiritual harm through coercion or shaming, legal exposure through improper medical claims, and reputational damage that weakens the broader pro-life witness. When training is mature, it forms volunteers who can speak carefully, serve consistently, and refer appropriately.
Volunteer training is a ministry of truth and care
Why training matters theologically
Pregnancy resource centers often serve at the intersection of crisis, shame, fear, and financial instability. Christian compassion in this setting is not sentiment; it is disciplined love. Scripture’s insistence on truthfulness is not suspended for a good cause. Christians are commanded to “speak the truth in love” (Ephesians 4:15), a standard that applies as much to counseling language and medical boundaries as it does to doctrinal teaching.
In practice, this means a center must train volunteers to communicate what the center actually provides, what it does not provide, and what it believes—without manipulation. The harder question is not whether a volunteer is pro-life; it is whether a volunteer can represent the ministry with integrity when a client is anxious, skeptical, or angry.
Why training matters legally and reputationally
Centers operate in a contested public environment. Many face scrutiny from regulators, journalists, and advocacy groups. Volunteer misstatements about medicine, confidentiality, or services offered can become the kind of incident that reshapes a donor’s confidence overnight. The Federal Trade Commission’s consumer protection mandate is broad, and false or misleading claims in any consumer-facing context can trigger serious consequences, especially if patterns appear across time. See the FTC’s consumer protection mission statement and enforcement posture at Federal Trade Commission.
Donors often assume risk is managed somewhere “in the back office.” In reality, much of a center’s risk management lives at the point of care: the greeter who promises something the center cannot deliver, the advocate who oversteps clinical boundaries, the mentor who mishandles a disclosure of abuse. Training is the center’s first serious line of protection for clients, volunteers, and the ministry’s witness.

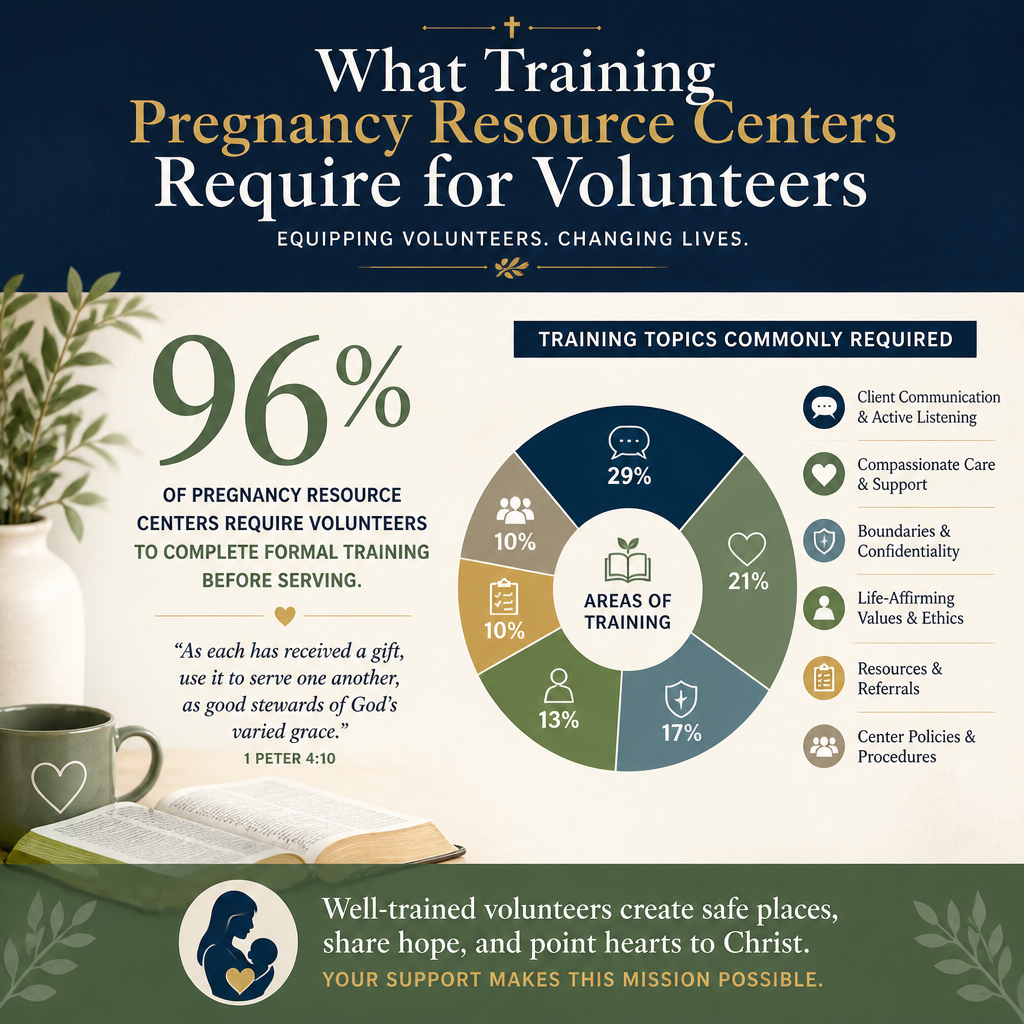
What strong pregnancy resource center training typically includes
Orientation and mission alignment
Most centers begin with a structured orientation that covers the center’s mission, statement of faith, client care philosophy, and service model. This is where donors should expect clarity about the center’s posture: a commitment to affirm the dignity of mother and child, to avoid pressure tactics, and to serve regardless of a client’s religious background.
Centers that hold up under scrutiny typically distinguish between pastoral care and client advocacy. They can articulate when prayer is offered, how it is offered, and how they respect a client who declines. This is not compromise. It is an application of neighbor-love that refuses to treat a vulnerable person as a project.
Confidentiality and mandated reporting
Confidentiality is among the most misunderstood aspects of pregnancy resource work. Volunteers must be trained in how the center handles client records, who may access them, what is shared with outside partners, and how limits of confidentiality are communicated. Training should also address mandated reporting requirements and the center’s protocol for suspected abuse or trafficking. Mandated reporting rules vary by state, but donors should expect the center to have written policies and regular refreshers, not informal guidance.
Boundaries and scope of practice
High-quality training spends significant time on boundaries: what a volunteer may say, what only licensed medical staff may say, and when to refer. This is especially important when a center provides ultrasound services. Ultrasound can be offered in a way that is clinically appropriate and ethically grounded, but the line between medical information and counseling persuasion must be carefully managed.
Many centers use a “warm referral” model—connecting clients to prenatal care, Medicaid enrollment support, housing assistance, domestic violence services, or licensed mental health care. A volunteer who understands boundaries is better able to serve a client with competence and humility rather than overpromising what the center can deliver.
Training differs by role and service model
Front desk and hospitality volunteers
Some roles appear simple but are often where trust is won or lost. Front desk volunteers need training in trauma-informed hospitality, de-escalation, and accurate representation of services. They should know how to handle protesters, hostile calls, and media inquiries without improvising. This is one place we see mature centers remove discretion from untrained volunteers by giving scripts and escalation pathways.
Client advocates and peer counselors
Client-facing advocates typically receive the most extensive training. Programs vary, but donors should expect material that covers active listening, motivational interviewing basics, grief and loss, domestic violence screening, sexual coercion, and cultural humility. A center may also train in sexual risk avoidance education, parenting support, and post-abortion support pathways.
Christians genuinely disagree about how explicitly pregnancy resource centers should engage contested moral questions in the counseling room. Some prefer direct moral language; others emphasize long-term relationship and incremental formation. The ministries that do this well are not those that avoid conviction, but those that can explain their approach, train for it, and hold volunteers accountable to it.
Medical volunteers and ultrasound teams
Where a center provides medical services, training should reflect clinical standards and state requirements. Licensed clinicians should be credentialed, and any volunteer support roles should be trained to avoid clinical interpretation. Donors should also look for protocols around infection control, patient privacy, documentation, and informed consent.
For donors who want a baseline sense of what legitimate clinical expectations look like, the U.S. Department of Health and Human Services offers extensive guidance on protecting health information under HIPAA at HHS. Not every center is a covered entity, but mature centers still treat privacy and documentation with seriousness that approximates clinical norms.
What donors can reasonably expect to see and verify
Training that is documented and repeatable
One-off lectures do not constitute a training system. Donors should expect documented training requirements, written policies, and periodic refreshers. The question is not whether every volunteer can quote the handbook; it is whether the center has defined standards and can show that volunteers were formed to meet them.
Across our verification work at Most Trusted, we find that centers with the strongest governance and lowest preventable risk tend to formalize volunteer onboarding, supervision, and re-authorization. They understand that good intentions do not replace systems.
Supervision, feedback, and corrective pathways
Training is only half the work. Ongoing supervision matters because real cases are complex. Donors should look for a clear chain of supervision, scheduled check-ins, and a documented pathway for addressing concerns. A center should be able to explain how it handles volunteer drift—when a volunteer begins to freelance with advice, theology, or medical claims.
Healthy centers also train volunteers in how to receive feedback. The aim is not control. It is the kind of humility Scripture commends: a willingness to be corrected for the sake of faithfulness and neighbor-love.
A short donor checklist
When assessing a center’s readiness, we recommend looking for the following indicators:
- Written role descriptions that clarify boundaries and supervision
- Documented onboarding and training requirements by role
- Confidentiality policies and a clear mandated reporting protocol
- Referral relationships that extend care beyond the center’s walls
- Ongoing supervision and periodic refresher training
If a center cannot answer these questions clearly, that does not automatically mean it is unfaithful. It may mean it has grown faster than its systems. Donors should not treat that as a small gap, because training gaps tend to surface at the most sensitive moments.
How training connects to trust and donor stewardship
Training as a transparency signal
Volunteer training is one of the most visible expressions of a center’s internal culture. A center that trains carefully is more likely to communicate honestly about outcomes, client feedback, and limits. It is also more likely to avoid the subtle temptation to treat numbers served as the primary measure of faithfulness.
This is where broader donor discernment comes into view. When donors explore Pregnancy Resource Centers, the strongest giving decisions often come from understanding not only what services are offered, but how they are offered and governed.
Training as a governance and integrity issue
Training requires money, staff time, and leadership attention. Some centers resist that investment because it feels “administrative.” But the modern nonprofit field has had to learn that formation and accountability are part of ministry, not distractions from it. The “Overhead Myth” letter—signed by leaders from GuideStar (now Candid), BBB Wise Giving Alliance, and Charity Navigator—helped correct the simplistic assumption that spending on systems is inherently suspect. See Candid’s discussion of the letter and its implications at Candid.
For pregnancy resource centers, training is one of those system investments that directly protects the mission. It reduces preventable errors, supports ethical communication, and increases the likelihood that clients experience consistent care across volunteer teams.
Donors who want to understand how volunteer formation fits into the broader ecosystem of service should also review Volunteering at Pregnancy Resource Centers, because volunteer structures often reveal whether a ministry’s compassion is sustained by thoughtful leadership or by constant crisis response.
FAQs for What training pregnancy resource centers require for volunteers
Do pregnancy resource center volunteers need formal counseling credentials?
Typically, no. Most centers rely on trained volunteers who are not licensed counselors, and that can be appropriate when the role is clearly defined, supervised, and bounded. What matters is that volunteers are trained to listen well, avoid clinical claims, and refer to licensed professionals when a client presents with trauma, severe mental health needs, domestic violence, or complex medical questions.
How long does volunteer training usually take at a pregnancy resource center?
It varies by role and by whether the center offers medical services. Some hospitality roles may require a shorter onboarding, while client advocate roles often require more extensive training and supervised observation before a volunteer meets with clients independently. Donors should be cautious of centers that cannot describe role-based training length and re-authorization practices, because unclear expectations often correlate with inconsistent client care.
A faithful center treats training as part of care
Pregnancy resource centers exist to offer practical help and moral clarity in moments when many women feel alone. Training is one of the primary ways a center honors that calling: by ensuring volunteers speak truthfully, respect boundaries, and serve with competence. Donors who want to give with confidence should treat volunteer training not as a minor operational detail, but as a measurable expression of integrity.



